
Translate this page into:
Once versus thrice daily dose regimen of gentamicin in abdominal surgery
*Corresponding author: John Adi Ashindoitiang, Department of Surgery, University of Calabar, Calabar, Cross River State, Nigeria. ashindoitiang90@yahoo.com
-
Received: ,
Accepted: ,
How to cite this article: Ashindoitiang JA. Once versus thrice daily dose regimen of gentamicin in abdominal surgery. Calabar J Health Sci 2023;7:99-103. doi: 10.25259/CJHS_47_2021
Abstract
Objectives:
The objectives of the study are to compare the effectiveness and likelihood of toxicity of 7.5 mg/kg single high dose and 80 mg thrice daily doses of intravenous gentamicin.
Material and Methods:
A total of 88 patients who had abdominal surgeries on account of acute abdomen infectious etiologies in a private hospital in Lagos, Nigeria, between August 2002 and July 2004 were studied. They were randomized into two groups (A and B), with each group comprising of 44 patients. Group A had 7.5 mg single high-dose gentamicin alongside cefuroxime for 5 days. Group B had 80 mg thrice daily of gentamicin for 5 days alongside cefuroxime. Renal function tests were carried out preoperatively and postoperatively. The surgical site infection rate was compared between Groups A and B.
Results:
There was statistically no significant difference in effectiveness and toxicity between the two groups except for severe infections in which 7.5 mg/kg body weight single high dose gentamicin was superior to 80 mg thrice daily doses. The infection rate was similar for both groups, and the organisms isolated in both groups were resistant to gentamicin. There was no difference in renal complication rate and ototoxicity. We also found that a single high dose was more convenient for nurses to administer, cost effective, decreased personnel time and had more patient comfort.
Conclusion:
A single high dose of gentamicin of 7.5 mg/kg daily is comparatively effective as 80 mg thrice daily dose. The infection rate was the same in both groups, with a single high dose much better in severe infection.
Keywords
Abdominal surgery
Gentamicin
therapy
Once versus thrice therapy

INTRODUCTION
Patients with acute abdomen comprise the largest group of people presenting as a general surgical emergency.[1] In the most acute abdomen, infection is the most common cause of acute appendicitis on the front burner.[1] The organisms involved are polymicrobial, with Gram-negative and Bacteroides as the most predominant, aminoglycosides of which gentamicin are a prototype in this class, and the most widely used are effective against Gram-negative infections. Hence, they form an integral part of the management of intra-abdominal infections despite their potential for nephrotoxicity and ototoxicity.[2] Nephrotoxicity occurs in 17%, while ototoxicity is observed in 8%, and vestibular functional impairment affects 3% of patients.[3] Several studies have compared a single daily dosing with multiple doses of aminoglycosides. Some of these studies showed single daily doses to be superior, while a few others showed multiple daily doses to be superior.[4,5] We compared the effectiveness of a single high dose of gentamicin and thrice daily dose in abdominal infections in patients that present with acute abdominal emergencies.
MATERIAL AND METHODS
A prospective single-blinded randomization was carried out. Consecutive patients who present with acute abdominal emergencies of infective origin were randomized into two groups (A and B). A total of 88 patients were seen during the study period of 2 years from August 2002 to July 2004 in a 75 bedded private hospital in Lagos, Nigeria. Group A had 44 patients who received a single high dose of gentamicin 7.5 mg/kg along with cefuroxime for 5 days. Group B patients received 240 mg daily doses of gentamicin in three divided doses alongside cefuroxime. For both groups, renal function was assessed before and after antibiotic treatments postoperatively by estimating urea, creatinine, sodium, potassium, bicarbonate, and chloride, while otovestibular function was assessed by asking the patients if they had tinnitus or noticed any change in their hearing abilities. Patients who had renal impairment with elevated creatinine >1 mg/dL were excluded, as well as patients who complained of hearing difficulties and childhood history of otitis media. Also excluded were patients younger than 16 years and those that weigh less than 50 kg. A patient who developed postoperative surgical site infection in both groups was evaluated with cultured/sensitivity patterns of the organisms isolated. For the purpose of this study, surgical site infection refers to the postoperative wound infection that occurs within 30 days following surgery for the acute abdomen.[6] Diagnosis is purely clinical, based on the Center for Disease Control and Prevention criteria for SSI.[6] Epi-fo 6 was used for statistical analysis. Infection rates between groups A and B were compared using Chi-square and a confidence interval set at 95% (CI) with statistical significance as P < 0.05.
RESULTS
A total of 88 patients were seen in Motayo Hospital, a 75-bed private hospital in Lagos, between August 2002 and July 2004. Patients who met the inclusion criteria were recruited into the study. Informed consent was obtained, and ethical approval was granted by the hospital management. The age range of the patients was between 16 years and 80 years, and a mean age of 46.96 ± 12.23 standard deviation. There were 50 males and 38 females, giving an M: F of 1.3:1 [Table 1 and Figure 1]. The diagnoses of the patients studied showed that acute appendicitis was the most frequent cause of acute abdomen, accounting for 56.82%. Intestinal obstruction was the second most frequent cause of acute abdomen, followed by complications of acute appendicitis and pelvic inflammatory disease, respectively (ruptured appendicitis and intra-abdominal abscesses) [Table 2]. The Group A patients (those who had a daily single-dose regimen of gentamicin alongside cefuroxime) are shown in Table 3, while the Group B patients (those who had 3 times daily doses regimen of gentamicin alongside cefuroxime) are shown in Table 4. The incidence of infections in both groups ranges from 27% to 50%. Infections were highest in patients with complicated colorectal malignancy and lowest with uncomplicated appendicitis. The Group A patients had an infection rate of 33.3% compared 40% infection rate for Group B patients with <0.003. Group A patients recorded no infection among patients with generalized peritonitis, while Group B patients with generalized peritonitis had a 33.3% rate with P < 0.001. Twenty five percent of Group A patients with intestinal obstruction had wound infection compared to 30% of Group B patients with P < 0.003. There was no difference in wound infection rates among the two groups in patients with acute appendicitis and colorectal cancer. The organisms isolated in various conditions showed that bacteroides were the most frequently isolated organism among the two groups [Table 5].
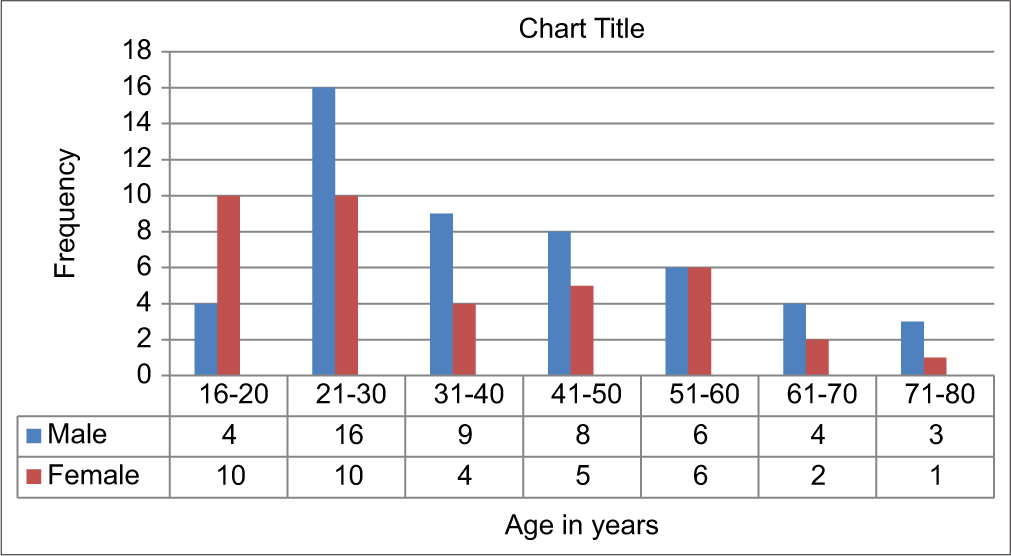
- Age and sex distribution.
| Diagnosis | Surgical procedure | Number | Percentages |
|---|---|---|---|
| Acute appendicitis | Appendectomy | 50 | 56.82% |
| Intestinal obstruction | Exploratory laparotomy | 18 | 20.45% |
| Generalized peritonitis 2° ruptured appendicitis | Exploratory laparotomy and appendectomy | 6 | 6.81% |
| Intra-abdominal abscesses | Exploratory laparotomy and drainage | 5 | 5.65% |
| Obstructed colorectal tumors | Hartman’s left and right hemicolectomy | 4 | 4.54% |
| Pancreatic abscess/necrosis | Exploratory laparotomy and debridement | 1 | 1.13% |
| Perforated gastric ulcer | Exploratory laparotomy and graham patch | 1 | 1.13% |
| Perforated DU | Same | 1 | 1.13% |
| Tubo-ovarian abscess | Drainage/tuboovarectomy | 1 | 1.13% |
| Perforated typhoid | Exploratory laparotomy and closure of perforations | 1 | 1.13% |
DU: Duodenal ulcer
| Diagnosis | Frequency | Percentages |
|---|---|---|
| Acute appendicitis | 25 | 56.82% |
| Intestinal obstruction | 8 | 18.18% |
| Generalized peritonitis 2° ruptured appendicitis | 2 | 4.54% |
| Intra-abdominal abscess | 3 | 6.81% |
| Obstructed colorectal cancer | 2 | 4.54% |
| Pancreatic A abscess/necrosis | 1 | 2.27% |
| Tubo-ovarian abscess | 1 | 2.27% |
| Perforated typhoid | 1 | 2.27% |
| Perforated gastric ulcer | 1 | 2.27% |
| Total | 44 | 100% |
| Diagnosis | Frequency | Percentages |
|---|---|---|
| Acute appendicitis | 25 | 56.81% |
| Intestinal obstruction | 10 | 22.72% |
| Generalized peritonitis | 4 | 9.09% |
| Intra-abdominal abscess | 2 | 4.54% |
| Obstructed colorectal cancer | 2 | 4.54% |
| Perforated DU | 1 | 2.27% |
| Total | 44 | 100% |
DU: Duodenal ulcer
| Procedure | Group A | Percentage | Group B | Percentage | Total for both groups | Overall infection rate |
|---|---|---|---|---|---|---|
| Acute appendicitis | 5/25 | 20% | 5/25 | 20% | 10/50 | 20% |
| Laparotomy for intestinal obstruction | 2/8 | 25% | 3/10 | 30% | 5/18 | 27% |
| Laparotomy for intra-abdominal abscess | 1/3 | 33.3% | 1/2 | 50% | 2/5 | 40% |
| Generalized peritonitis | 0/2 | Nil | 2/4 | 50% | 2/6 | 33.3% |
| Colorectal | 1/2 | 50% | 1/2 | 50% | 2/4 | 50% |
| Total | 9 | 20.4% | 10 | 22.7% | 21 | 23.8% |
| Diagnosis | Organism isolated | Sensitivity |
|---|---|---|
| Acute appendicitis | 1. Strept faecalis | Dicloxacillin |
| 2. Baceroides | Flagyl | |
| Intra-abdominal abscess | Bacteroides | Flagyl |
| Intestinal obstruction | Enterococcus | Co-trimazole |
| Generalized peritonitis | Bacteroides | Flagyl |
| Colorectal cancer | Clostridium species | Penicillin crystalline |
DISCUSSION
Acute abdomen is a common surgical emergency with multifactorial etiologies. It constitutes a major part of a surgeon’s clinical workload and is one of the most demanding and sometimes with less fantastic outcomes areas of surgical practice.[7] There are often progressing underlying complications such that undue delay in management may affect the final prognosis. Infection is the most common cause of acute abdomen in the form of acute appendicitis. In both developed and developing countries, acute appendicitis is the most common surgical emergency.[8,9] In Nigeria, acute appendicitis is reported to be the most common surgical abdominal emergency.[10] In this study, it accounts for over half of cases with surgical abdominal infections. Due to delay in presentation in our environment, there is a higher incidence of complication, which constitutes up to another 10–12% of causes of surgical abdominal infections seen in this study. Other causes of acute abdomen in the study show intestinal obstruction, accounting for 20–25% adhesive bowel obstruction and obstructing colorectal cancer, gynecological causes, acute pancreatitis, perforated peptic ulcer, and perforated typhoid. The pattern seen in this study is similar to the spectrum of acute abdominal pain and has the same features with study done in Ghana.[7] Surgical abdominal infections are polymicrobial, with some series reporting up to 14 different organisms cultured in patients with perforated appendicitis.[11] The most common organisms seen in acute and ruptured appendicitis are Escherichia coli and Bacteroides. Varieties of other Gram-negatives are involved, and the same flora seen in acute appendicitis is involved in other abdominal infections. Aminoglycosides have potent activity against Gram-negative bacteria and are often used to treat infections caused by these species, especially when resistance to beta-lactam antibiotics is suspected.[12] A once-daily dose is more convenient and has been proposed to be equally effective and potentially less toxic than multiple doses.[13-16]
In this study, we compared a daily single high dose of gentamicin 7.5 mg/kg body weight alongside cefuroxime with a thrice 800 mg daily dose of gentamicin alongside cefuroxime. The study showed a slight difference in clinical efficacy. The group with high single-daily doses of gentamicin had an overall infection rate of 20.4%, while thrice-daily gentamicin group had a 22.7% infection rate. There was no difference in toxicity between the two groups, as no patients showed any difference between preoperative and postoperative renal function. Furthermore, no patient reported any observation of a change in vestibuloauditory function. Once daily dose shows better results in severe infections such as intra-abdominal abscess and generalized peritonitis. The incidence of infection according to classification was clean wounds at 1.5%, clean contaminated wounds at 9%, contaminated wounds at 20%, and dirty wounds at 43%.[17] Although there has been a decrease with the advent of more potent antibiotics, the infection rate in the study is well within the expected range.
The wound infection rate would have been lower if metronidazole had been added to the regimen, as the common isolate was bactericides.
CONCLUSION
The complication rate was high in our study compared with findings from previous studies; this is most likely due to our observation of delayed patient presentation to the hospital. There was a slight difference in clinical efficacy, with the rate of wound infection slightly higher in patients who had thrice daily doses of gentamicin alongside cefuroxime. Dirty and contaminated wounds were the most frequent wound infections compared to clean, contaminated wounds.
Ethical approval
The research/study was approved by the Instiutional Ethics committee of University of calabar, approval number UCTH/HEC/331/VOL/111/354 dated 5th May, 2021.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Review of the pathological results of 2660 appendectomy specimen. J Gastroenterol. 2006;41:745-9.
- [CrossRef] [PubMed] [Google Scholar]
- Once versus thrice daily gentamicin in patients with serious infections. Lancet. 1993;34:335-41.
- [CrossRef] [PubMed] [Google Scholar]
- Aminoglycosides toxicities a review of clinical studies between 1974 and 1980. J Antimicrob Chemother. 1984;13:9-22.
- [CrossRef] [PubMed] [Google Scholar]
- Single or multiple daily doses of aminoglycosides: A meta-analysis. BMJ. 1996;312:338-45.
- [CrossRef] [PubMed] [Google Scholar]
- Comparative trial of single dose versus twice daily sisomicin in bacteriuric patients. J Clin Pharmacol. 1977;17:520-8.
- [CrossRef] [PubMed] [Google Scholar]
- Epidemiology of myelomeningocoele in Africa: An experience in a Regional Neurosurgical Center in Northern Nigeria. J Pediatr Neurosci. 2022;17:237-43.
- [CrossRef] [Google Scholar]
- Clinical spectrum of acute abdominal pain in Accra, Ghana. West Afr J Med. 1999;18:13-6.
- [Google Scholar]
- Acute surgical admission for abdominal pain in adults in Kumasi, Ghana. ANZ J Surg. 2006;76:898-903.
- [CrossRef] [PubMed] [Google Scholar]
- Tropical surgical abdominal emergencies: Acute appendicitis. Trop Geogr Med. 1989;41:118-22.
- [Google Scholar]
- Bacteriology of histopathologically defined appendicitis in children. Pediatr Infect Dis. 2000;19:1078-83.
- [CrossRef] [PubMed] [Google Scholar]
- Aminoglycosides: Single or multiple daily dosing? Lancet. 1993;341:1152.
- [CrossRef] [PubMed] [Google Scholar]
- Once-daily aminoglycoside therapy. Antimicrob Agents Chemother. 1991;35:399-405.
- [CrossRef] [PubMed] [Google Scholar]
- Single daily dose therapy with aminoglycosides. J Hosp Infect. 1991;18:117-29.
- [CrossRef] [PubMed] [Google Scholar]
- Once-daily versus thrice-daily dosing of netilmicin in combination with beta-lactam antibiotic as empirical therapy for febrile neutropenic patients. J Antimicrob Chemother. 1993;31:585-98.
- [CrossRef] [PubMed] [Google Scholar]
- Single or multiple daily doses of aminoglycosides: A meta-analysis. BMJ. 1996;312:338-45.
- [CrossRef] [PubMed] [Google Scholar]
- The epidemiology of wound infection: A ten year prospective study of 62,939 wounds. Surg Clin North Am. 1980;60:27-40.
- [CrossRef] [PubMed] [Google Scholar]




