
Translate this page into:
A review of endoscopic findings in upper gastrointestinal bleeding in Calabar, South-South Nigeria: A two-center study
 , Uhegbu Kelechi3, Itam-Eyo Asa E1, Eko Benedicta A4, Effiong Esther I4, Ndoma-Egba Rowland2
, Uhegbu Kelechi3, Itam-Eyo Asa E1, Eko Benedicta A4, Effiong Esther I4, Ndoma-Egba Rowland2

*Corresponding author: Mbang Kooffreh-Ada, Department of Internal Medicine, University of Calabar, Calabar, Nigeria. mkooffreh@yahoo.com
-
Received: ,
Accepted: ,
How to cite this article: Kooffreh-Ada M, Ngim OE, Okonkwo UC, Chukwudike ES, Ikobah JM, Uhegbu K, et al. A review of endoscopic findings in upper gastrointestinal bleeding in Calabar, South-South Nigeria: A two-center study. Calabar J Health Sci 2023;7:93-8. doi: 10.25259/CJHS_7_2024
Abstract
Objectives:
Upper gastrointestinal bleeding (UGIB) is a leading cause of mortality and morbidity in Nigeria. Endoscopy is vital for the diagnosis of UGIB. At present, there are no published data on UGIB in Cross River State, Nigeria. This study aims to report the endoscopic findings in our patients with UGIB in Calabar, Cross River State (CRS).
Material and Methods:
This was a retrospective study of patients with UGIB who had esophagogastroduodenoscopy (EGD) performed at two health facilities in Calabar, CRS, from November 2012 to May 2024. Patients’ demographics and endoscopic findings were obtained from the endoscopy registers into a spreadsheet and analyzed statistically (using the Statistical Package for Social Sciences version 20 software). Summary statistics (means ± standard deviation [SD]) for continuous variables and frequencies and percentages for categorical variables were analyzed. Categorical variables were compared for differences using the chi-square test or Fisher’s exact test.
Results:
A total of 923 EGDs were performed during the study period. 151 (16.4%) of these cases had UGIB as an indication for the procedure. There were 105 males (69.5%) and 46 females (30.5%) with a mean age of 47.5 (SD ± 17.9) years. Peptic ulcer disease (PUD) (gastritis and benign gastric ulcer – 68, 45%) was the main pathology found in patients, followed by bleeding esophageal varices (33, 21.9%).
Conclusion:
Endoscopy is important in the diagnosis of UGIB. PUD and bleeding esophageal varices are the leading causes of UGIB in our environment, respectively.
Keywords
Calabar
Esophagogastroduodenoscopy
Esophageal varices
Peptic ulcer disease
Upper gastrointestinal bleeding

INTRODUCTION
Upper gastrointestinal bleeding (UGIB) is a common clinical presentation often seen in gastroenterology practice. It is associated with significant morbidity and mortality rates, especially in regions where healthcare resources are limited. The morbidity and mortality rates are understandably higher in resource-poor settings where infrastructure and the required equipment, as well as trained medical personnel, necessary for the management of this condition are limited.[1] UGIB is defined as blood loss within the lumen of the digestive tract proximal to the ligament of Treitz.[2]
The etiology of UGIB can be broadly classified into variceal (esophageal and gastric varices) and non-variceal (peptic ulcer disease [PUD], gastroduodenal erosions, tumors, Mallory– Weiss tear, etc.).[2,3] Regarding the global epidemiology of UGIB, up to 50% of cases arise from PUD, especially in developed countries, followed by esophageal varices, seen mostly in low-income nations.[3-5] The global incidence rates of UGIB range from 48 to 170 cases per population per annum, and UGIB is the leading indication for upper gastrointestinal (GI) endoscopy in Nigeria and globally.
Esophageal varices are dilated submucosal distal esophageal veins connecting the portal and systemic circulations arising from portal hypertension (especially from liver cirrhosis), resulting in resistance to portal blood flow and increased portal venous blood inflow. This raised venous pressure causes the development of portosystemic collaterals, which can eventually rupture and bleed.[6] While, bleeding arising from PUD occurs when the ulcer erodes into a sub-epithelial blood vessel.[7] Presentation ranges from oozing from smaller caliber mucosal capillaries to more brisk bleeding from larger caliber arterial branches.[7] Shallow mucosal erosions and ulceration can also result in less dramatic bleeding from the upper-, mid-, and lower-GI tract, resulting in iron deficiency anemia.[7] The clinical presentation of UGIB may include hematemesis, melena, hematochezia, syncope, or shock. It is more common in males and older adults.[8,9]
UGIB is 4 times as common as lower GI bleeding.[10] Lower GI bleeding is less severe than UGIB and it is often a self-limiting condition. Most UGIB patients are managed conservatively, using endoscopy, while only a third of patients with lower GIB are treated endoscopically.[10] Esophagogastroduodenoscopy (EGD) is the diagnostic modality of choice for UGIB, with more sophisticated investigations such as computed tomographic angiography and capsule endoscopy being indicated when endoscopy is inconclusive.[2,9]
Considering the pivotal role endoscopy plays in the diagnosis and management of GI conditions such as UGIB, it is then reasonable to recommend the widespread use of this technology in gastroenterology practices across the country. Although endoscopic services have been available in Calabar, Cross River State (CRS) for over a decade now, no study has reported the endoscopic findings (causes) of UGIB. Understanding the diseases responsible for UGIB in our environment can help further contribute to the knowledge of this condition in the country as well as offer a definitive diagnosis with a minimally invasive approach. This can lead to the prompt and appropriate management of patients, which may save them from months or years of unnecessary illness or anxiety.
MATERIAL AND METHODS
This was an observational study designed as a retrospective evaluation of patients referred to the endoscopy unit of the University of Calabar Teaching Hospital (UCTH) and a private clinic based in Calabar metropolis (Jil Specialist Clinic) in South–South Nigeria over a 12-year (November 2012–May 2024). These health facilities provide specialist care in gastroenterology and endoscopy. The UCTH is a 780-bed capacity tertiary center providing tertiary-level health care within CRS and its environs. The hospital is a major referral center in the state, offering a wide range of specialist health care, including gastroenterology and endoscopic services. JIL Specialist Clinic is a private clinic in the Calabar metropolis that also offers gastroenterology, surgical, and endoscopic services. An Olympus 190 series video gastroscope system was used for patients in the endoscopy unit of the UCTH, whereas an Olympus 140 series video gastroscope was used for patients who had their endoscopy at the JIL Specialist Clinic. The procedure was performed as day cases in both facilities. All patients were duly counseled about the procedure and informed consent was subsequently obtained. The patient’s vital signs and oxygen saturation were routinely monitored before, during, and shortly after the procedure. Patients had an overnight fast before the procedure, with an occasional few having a minimum of 6–8 hours fast. Local anesthesia was achieved using 10% xylocaine pharyngeal spray. In a few selected cases, conscious sedation by an anesthetist was provided. Upper GI endoscopy was carried out with the patient lying in the left lateral position. Endoscopic evaluation of bleeding PUD was defined according to the Forrest classification system as follows: FI (FIa and FIb), FII (FIIa, FIIb, and FIIc), and FIII.[1] Patients who had esophageal variceal bleeding were classified endoscopically according to Paquet’s grading of esophageal varices, that is, I–IV.[9] The endoscopic diagnosis of the etiology of UGIB was made once there was evidence of active or recent bleeding, irrespective of the nature of the bleeding lesion. Normal findings were defined by the absence of any endoscopic abnormality.[1]
Data was obtained from the endoscopy suite register of UCTH and Jil Specialist Clinic from the time endoscopy services began in either centers i.e. November 2012 to May 2024 (twelve years). The information obtained from the patients was anonymous. No patients were involved in developing the research process and informed consent forms were not required in this retrospective study. The study was approved by the Health Research Ethics Committee (HREC) of the UCTH. The HREC protocol assigned number was UCTH/HREC/33/Vol.III/342. Trained research assistants investigated required documentation and information on age, sex, and endoscopic diagnosis.
Data entry and analysis were carried out through the use of the Statistical Package for the Social Sciences version 20. The variables studied include demographics of patients, clinical presentation, and endoscopic findings. Univariate analysis was carried out on all the sociodemographic, clinical, and endoscopic findings of patients presenting with UGIB.
RESULTS
Demographics and clinical features of study participants
One thousand five hundred and sixty-three patients underwent upper and lower GI services during the study period, out of which 923 patients had UGIE performed. One hundred and fifty-one (16.4%) of these cases had UGIB as an indication for the procedure. There were 105 males (69.5%) and 46 females (30.5%) with a mean age of 47.5 (standard deviation [SD] ± 17.9) years. The ratio of male-to-female was 2.3:1 [Table 1].
| Variable | UGIB | UGIB |
|---|---|---|
| n=151 | Frequency (%) | |
| Age (years) | ||
| <18 | 6 | 4 |
| 18–45 | 62 | 41.1 |
| 46–64 | 55 | 36.2 |
| >65 | 28 | 18.5 |
| Gender | ||
| Male | 105 | 69.5 |
| Female | 46 | 30.5 |
Endoscopic findings in patients with UGIB
The endoscopic findings in patients with UGIB are shown in Figure 1. Endoscopic abnormalities that were present include benign gastric/duodenal peptic ulcers (68, 45.0%), esophageal varices (33, 21.9%), gastroduodenal malignancies (9, 6.0%), normal findings (8, 5.3%), and other etiologies (19, 12.6%). Only 8 patients (24.2%) with esophageal varices underwent endoscopic variceal band ligation (EVL). One patient was hemodynamically unstable, and the procedure had to be terminated. Four patients had colonoscopies done to evaluate the UGIB further [Figure 1].
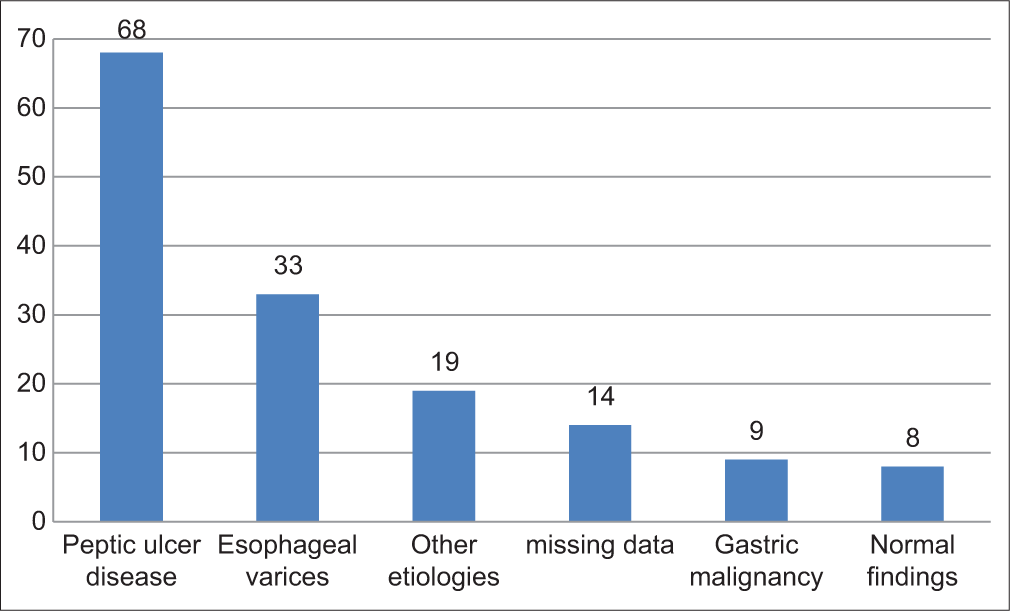
- Endoscopic findings in patients with upper gastrointestinal bleeding.
Endoscopic findings in patients with other etiologies
These include severe gastritis/gastric erosions (12, 63.2%), severe esophagitis/esophageal tumors (5, 26.3%), Diuelafoy’s lesion (1, 5.3%), and angiodysplasia (1, 5.3%) [Figure 2].
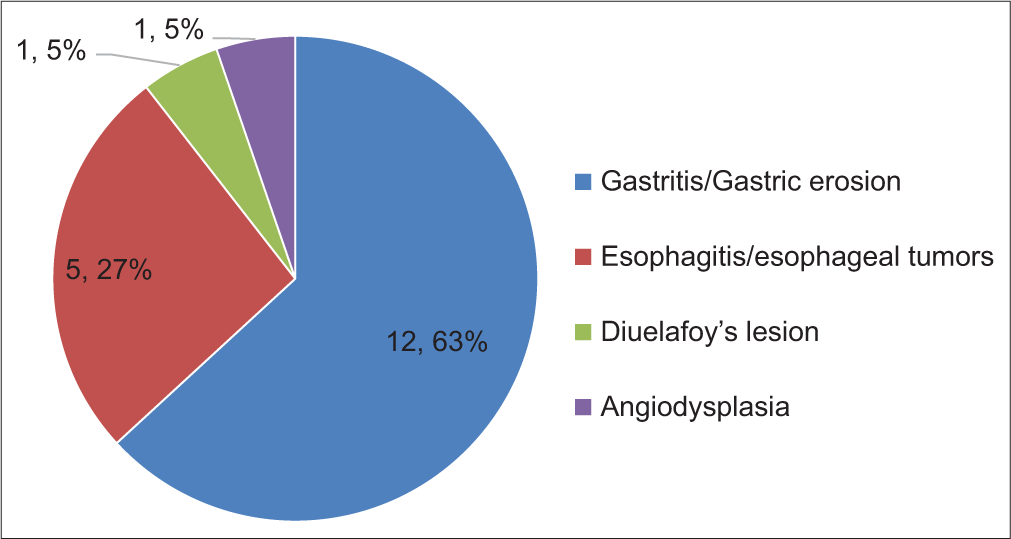
- Endoscopic findings in patients with other etiologies.
Distribution of UGIB in patients based on age and gender subgroups
Male patients were mostly found to have the leading causes of UGIB, that is, PUD (64.7%) and esophageal varices (81.8%), though this was not statistically significant. Among the age sub-groups, patients aged between 45 and 64 years mostly had PUD (39.1%), whereas patients aged between 18 and 44 had esophageal varices (60.6%) [Table 2].
| Variable | Male (%) | Female (%) | P-value | <18 years (%) | 18–44 years (%) | 45–64 years (%) | >65 years (%) | P-value |
|---|---|---|---|---|---|---|---|---|
| PUD (68) | 44 (64.7) | 24 (35.3) | 3 (5.8) | 23 (33.3) | 27 (39.1) | 15 (21.7) | ||
| EV (33) | 27 (81.8) | 6 (18.2) | 0.614* | 1 (3.0) | 20 (60.6) | 9 (27.3) | 3 (9.1) | 0.660* |
| Gastriccancer(9) | 6 (66.7) | 3 (33.3) | 0 (0) | 4 (44.4) | 3 (33.3) | 2 (22.2) | ||
| Normal (8) | 5 (62.5) | 3 (37.5) | 0 (0) | 4 (50.0) | 3 (37.5) | 1 (12.5) |
DISCUSSION
Despite the challenges low-resource environments face in scaling up endoscopic services, the advent of this service (therapeutic and diagnostic) in gastroenterology practice in Nigeria in the past decades has played a pivotal role in managing patients with UGIB bleeding. Nigerian healthcare providers are now better equipped to make informed patient triage/evidence-based decisions for appropriate clinical intervention, thus eliminating hypothetical practices. UGIB is a common indication for endoscopy. In our study, a total of 923 EGDs were performed, of which 16.4% of cases had UGIB as an indication for UGIB. This was slightly less than other studies conducted in bigger cities in the county, with EGD being performed in patients with UGIB ranging from 12% to 37%.[1,8,11] The variations in the number of EGD cases performed could be a result of the availability of funds, population density, relative prevalence of UGIB, and availability of appropriate expertise, among other factors.[12]
Most of the patients with UGIB fell between the age of 18– 44 years with a mean age of 47.5 (SD ± 17.9) years, while more males had the procedure done when compared to females with a male-to-female ratio of 2.3:1. This finding reflected a predominantly young male demographic picture that is comparable with other studies done across the country.[1,8,11] The male preponderance seen in our study may be explained by the higher tendency of Nigerian males to indulge in alcohol consumption and smoking, as well as being prone to underlying conditions such as PUD and chronic liver disease (CLD).[8] In addition, patients aged between the fifth and seventh decade (45–64 years) of life were the next age category to have UGIB. This rising trend of UGIB with increasing age appears to be common.[8] The frequent use of non-steroidal anti-inflammatory drugs for their anti-antithrombotic effect for the prevention of adverse cardiovascular events (such as stroke and ischemic heart disease), treatment of arthritis, and other rheumatologic symptoms have been cited as reasons for this rising trend in older age groups.[7,8] Our study demonstrated that PUD (45.0%) was the main pathology seen in patients with UGIB. Ngim et al. reported a similar finding in a preliminary report of upper GI endoscopy in Calabar. PUD (gastritis, duodenitis, benign gastric, and peptic ulcer) was the leading condition seen during the procedure.[12] This finding was comparable with other studies carried out in southern Nigeria.[1,2,8,11] The high burden of PUD in our study may not be surprising in our environment. In a previous study conducted in dyspeptic patients in Calabar, the presence of Helicobacter pylori (h. pylori) infection was relatively high following urea breath test analysis.[13] In a recent local study conducted in patients with h. pylori infection, EGD findings confirmed the important role of this gram-negative bacilli in the pathogenesis of PUD.[14] The burden of h. pylori in Africa is reported to be high in comparison to advanced countries, this may not be unusual considering the feco-oral route of transmission of this pathogen.[13] In contrast, Yayha et al. in Northern Nigeria reported esophageal and gastric varices as the leading cause of UGIB in their patients who had upper GI performed, this was also reported by Manko et al.[3,10] The high prevalence of hepatitis B and C with resultant chronic liver disease in the northern part of Nigeria may be a plausible explanation for the regional variation observed in the etiology of UGIB between the north and south of the country.[3,10,15] Chronic liver disease plays a significant role in the pathophysiology of portal hypertension and this in turn predisposes to varices.[3,10,15] CLD plays a significant role in the pathophysiology of portal hypertension, and this, in turn, predisposes to varices.[15] Reports from East Africa (Uganda and Malawi) also found varices to be a leading cause of UGIB among their patients.[4,16] Manko et al. adduced another reason for the high burden of CLD in the northern parts of Nigeria to the exposure to parasitic infestations from schistosomiasis.[3] They noted that most of the Northern populace are farmers many of whom practice irrigation farming. This farming method increases their risk of acquiring schistosomal infestation and subsequent hepatic schistosomiasis, contributing to the burden of CLD in the region.[3]
Regarding the severity of PUD and esophageal varices in our UGIB patients, the majority (30, 61.2%) of the PUD patients had clean-based benign ulcers, that is, Forrest class 3 [Table 3].[1] These categories of patients were referred to the gastroenterology clinic for conservative management utilizing a urea breath test or H. pylori stool antigen test for the detection of H. pylori and subsequent eradication of the infection. None of them had a repeat EGD (second-look endoscopy) for re-evaluation. Alatise et al. observed in their study that the majority of their patients with bleeding PUD had Forrest class 2C (hematin-covered flat spot).[1] The majority of their patients with UGIB were managed conservatively.[1] Endoscopic treatment is indicated for ulcers with active bleeding or a visible non-bleeding vessel.[17] Endoscopic treatment is largely not recommended for ulcers with hematin on the ulcer base or a clean ulcer base.[17] The risk of re-bleeding in patients with Forrest class 2C and 3 without endoscopic intervention is low.[18] Second look endoscopy is defined as routine endoscopy after initial hemostatic therapy.[17] It has been shown that the conservative treatment with a high intravenous dosage of proton pump inhibitors is as effective as second look endoscopy in reducing re-bleeding. Hence, routine second-look endoscopy after initial endoscopic hemostasis is not recommended and should be reserved for patients with a high risk of re-bleeding.[17] Endoscopic treatment of bleeding PUD is constrained in our environment due to the non-availability of medical supplies/equipment such as injection (epinephrine and sclerosants), thermal devices (heater probe and argon plasma coagulation), and mechanical therapy (clips). Our study demonstrates that endoscopy plays an important role in the management and stratification of bleeding PUD. This can greatly improve the management of our patients with the advantage of being cost-effective and definitive, especially in those with low risk of re-bleeding. In our patients who had UGIB from bleeding esophageal varices, the majority of them had grade III varices, which suggests that most of the patients had late presentation of liver cirrhosis. A typical finding in Nigeria where hepatitis B and C are the leading causes of CLD due to the endemic nature of the infection.[19] Another reason for this finding may be the delay in the performance of UGIE in liver cirrhosis patients who are prone to varices from portal hypertension.[8] Only 8 out of the 33 patients (24.2%) had EVL performed. Alatise et al. offered a higher number of patients (45 out of 52–87%) endoscopic treatment with either injection sclerotherapy or EVL. More than a third (28.8%) of their patients had injection sclerotherapy done.[1] Injection sclerotherapy is a more affordable endoscopic hemostatic technique in variceal bleeding when compared to EVL. However, it has been largely replaced by EVL, which has fewer re-bleeding episodes and adverse events.[20] The relatively low uptake of EVL in our environment is due to the high cost of the procedure, which most of our patients are unable to afford.
| Variable | Frequency | Percentage |
|---|---|---|
| Forrest classification (n=49) | ||
| 1A(Spurtingbleed) | 0 | 0 |
| 1B(Oozingbleed) | 15 | 30.6 |
| 2A(Non-bleedingvisiblevessel) | 2 | 4.1 |
| 2B(Adherentclot) | 2 | 4.1 |
| 2C(Hematincoveredflatspot) | 0 | 0 |
| 3 (Clean-based ulcer with no signs of bleeding) | 30 | 61.2 |
| Missingdata(19) | ||
| Grade of Esophageal Varices (n=29)* | ||
| GradeI–Microcapillarieslocated in the distal esophagus or esophago-gastric junction | 5 | 17.2 |
| GradeII–Oneortwosmallvarices located in the distal esophagus | 6 | 20.7 |
| GradeIII–Medium-sizedvarices of any number. | 13 | 44.8 |
| GradeIV–Large-sizedvaricesin any part of the esophagus | 4 | 13.8 |
| Esophageal varices and duodenal ulcer | 1 | 3.4 |
| Missing data (4) | ||
Our study revealed the significant value of endoscopy in detecting other serious conditions responsible for UGIB such as gastric and esophageal malignancy seen in 9 (6.0%) and 5 (3.3%) of our patients, respectively. In addition, identifying rare causes of UGIB such as Dieulafoy’s lesion (1, 0.7%) and angiodysplasia (1, 0.7%). It further availed us the opportunity to obtain tissue by biopsy, for histological diagnosis of cancer, thereby offering patients a holistic approach to their care.
Limitations
Because of the retrospective nature of our study, we could not ascertain the time from the presentation with UGIB to the performance of endoscopy. In addition, there were missing data in a few patients due to the manual entry of our data.
Recommendation
We recommend the use of modern digital reporting and the entry of endoscopic findings using validated endoscopy software in keeping with international best practices. This ensures appropriate entry and retrieval of data. The information generated can be useful for future research in the field of endoscopy as well as provide evidence-based resources for the design of guidelines peculiar to our environment. In addition, due to the high cost of endoscopic services in Nigeria, we recommend that endoscopic services should be covered in health insurance schemes across the country to reduce out-of-pocket expenses for patients. Furthermore, the government needs to improve funding of health services in the country through capacity building by training medical personnel in the field of therapeutic/interventional endoscopy as well as upgrades of medical infrastructure in the field.
CONCLUSION
The findings from this two-center study demonstrate that UGIB is an important indication for endoscopy. Our findings are comparable with other studies from public institutions across the country. PUD and esophageal varices are the most common endoscopic findings seen in UGIB patients in Calabar.
Acknowledgment
I wish to thank the entire members of the endoscopy unit for the teamwork and professionalism they display as well as the team of Biomedical Engineers who ensure that our endoscopy machines work optimally. I sincerely thank my colleagues in the anesthesia department who have continued to support our unit in delivering expert care to our patients.
Ethical approval
The research/study was approved by the Health Research Ethics Committee Board (HREC) of the University of Calabar Teaching Hospital. The HREC protocol assigned number was UCTH/HREC/33/111, dated 15th January, 2021.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript, and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Management of overt upper gastrointestinal bleeding in a low resource setting: A real-world report from Nigeria. BMC Gastroenterol. 2014;14:210.
- [CrossRef] [PubMed] [Google Scholar]
- Endoscopic findings in patients with upper gastrointestinal bleeding in Ogun state, Nigeria. Cureus. 2022;14:e23637.
- [CrossRef] [PubMed] [Google Scholar]
- Demographic profile and endoscopic findings among patients with upper gastrointestinal bleeding in Ahmadu Bello University Teaching Hospital, Zaria, NorthWestern Nigeria. Niger J Clin Pract. 2020;23:1163.
- [CrossRef] [PubMed] [Google Scholar]
- The role of endoscopy after upper gastrointestinal bleeding in sub-Saharan Africa: A prospective observational cohort study. Malawi Med J. 2020;32:139-45.
- [CrossRef] [PubMed] [Google Scholar]
- Pharmacogenomics of NSAID-induced upper gastrointestinal toxicity. Front Pharmacol. 2021;12:684162.
- [CrossRef] [PubMed] [Google Scholar]
- Esophageal varices In: StatPearls. Treasure Island, FL: StatPearls Publishing; 2023. Available from: https://www.ncbi.nlm.nih.gov/books/NBK448078 [Last accessed on 2024 Jul 07]
- [Google Scholar]
- Non-steroidal anti-inflammatory drugs and the gastrointestinal tract. Clin Med. 2021;21:131-4.
- [CrossRef] [PubMed] [Google Scholar]
- Upper gastrointestinal bleeding in a Nigerian diagnostic center: A retrospective study of endoscopic records. Ann Afr Surg. 2022;19:28-32.
- [CrossRef] [Google Scholar]
- Upper and lower gastrointestinal bleeding: A retrospective study on 10 years experiences in Southeastern Iran. Middle East J Dig Dis. 2023;15:116-20.
- [CrossRef] [PubMed] [Google Scholar]
- Endoscopy for upper gastrointestinal bleeding in a tertiary hospital in Kaduna, North-West Nigeria: Experience and findings. Ann Afr Med. 2022;21:262.
- [CrossRef] [PubMed] [Google Scholar]
- Endoscopic evaluation of upper and lower gastrointestinal bleeding. Niger J Surg. 2015;21:106-10.
- [CrossRef] [PubMed] [Google Scholar]
- A two-year review of upper gastrointestinal endoscopy in Calabar, Nigeria. IOSR J Dent Med Sci. 2017;16:31-4.
- [CrossRef] [Google Scholar]
- Prevalence of Helicobacter pylori infection among dyspepsia patients in Calabar. Glob J Pure Appl Sci. 2019;25:145-51.
- [CrossRef] [Google Scholar]
- Spectrum of endoscopic findings in patients with Helicobacter pylori infection in a Nigerian tertiary institution. Niger J Gastroenterol Hepatol. 2023;15:27.
- [CrossRef] [Google Scholar]
- Etiology of upper gastrointestinal bleeding in the University of Benin Teaching Hospital, South-Southern Nigeria. Niger J Surg Sci. 2016;26:29.
- [CrossRef] [Google Scholar]
- Endoscopic findings in upper gastrointestinal bleeding patients at Lacor hospital, Northern Uganda. Afr Health Sci. 2013;12:518-21.
- [CrossRef] [PubMed] [Google Scholar]
- Endoscopic management of peptic ulcer bleeding. Clin Endosc. 2015;48:106-11.
- [CrossRef] [PubMed] [Google Scholar]
- The recurrent bleeding risk of a Forrest IIc lesion at the second-look endoscopy can be indicated by high Rockall scores = 6. Surg Endosc. 2020;34:1592-601.
- [CrossRef] [PubMed] [Google Scholar]
- Risk factors of chronic liver disease amongst patients receiving care in a Gastroenterology practice in Calabar. IOSR J Dent Med Sci. 2015;14:6-13.
- [Google Scholar]
- Diagnosis and management of esophagogastric varices. Diagnostics. 2023;13:1031.
- [CrossRef] [PubMed] [Google Scholar]




