
Translate this page into:
Assessment of radiation equivalent dose to pediatric patients during chest radiography
 , Ekaete V. Ukpong2, Emmanuel O. Esien-Umo2, Blessing Ibe2, Andrew W. Ijever2, Akwa Egom Erim2,, Samson O. Paulinus2
, Ekaete V. Ukpong2, Emmanuel O. Esien-Umo2, Blessing Ibe2, Andrew W. Ijever2, Akwa Egom Erim2,, Samson O. Paulinus2

*Corresponding author: Akwa Egom Erim, Department of Radiography and Radiological Science, University of Calabar, Calabar, Cross River State, Nigeria. erimakwa@unical.edu.ng
-
Received: ,
Accepted: ,
How to cite this article: Inah GB, Ukpong EV, Esien-Umo EO, Ibe B, Ijever AW, Erim AE, et al. Assessment of radiation equivalent dose to pediatric patients during chest radiography. Calabar J Health Sci 2022;6:88-91.
Abstract
Objectives:
The study investigated the equivalent dose delivered during pediatric chest radiography.
Material and Methods:
This study adopted a prospective and cross-sectional research design and was conducted between April 26 and July 2, 2021, at the University of Calabar Teaching Hospital, Calabar, Cross river state, Nigeria. A total of 85 pediatric patients aged 0–15 years, referred for chest X-ray examination, were recruited into the study. The chest radiography was taken for each child in erect or supine positions. Children, who needed some form of immobilization, were immobilized and respiration (breathing) was observed to take exposures at end-expiration. Exposure factors used ranged between 40 and 80 kVp, 1–2 mAs, source-to-image distance; 110 cm. Patient demographics and chest X-ray exposure factors for each exposure were recorded using a spreadsheet. The equivalent dose was calculated using the NUTECHRX software version. All statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS) version 21.0. Statistical significance was set at P < 0.05.
Results:
The estimated mean equivalent dose was 0.0046 ± 0.0026 mSv, while the mean of weight (kg), kVp, and mAs was 15.04 ± 14.51 kg, 58.28 ± 10.58V, and 1.79 ± 1.56 mAs, respectively. Mean equivalent dose was 0.00447mSv (uncertainty 0.0027) for female and 0.00464mSv (uncertainty 0.0026) for male, with no significance difference between them. The mAs showed strong positive correlation with equivalent dose (r = 0.71, P = 0.05), while weight demonstrated a strong negative correlation with equivalent dose (r = −0.98, P = 0.05).
Conclusion:
Current-time product (mAs) and the weight of a child are important determinants of equivalent dose in pediatric chest radiography.
Keywords
X-radiation
Equivalent dose
Pediatric
Chest X-ray

INTRODUCTION
Radiation protection in pediatric patients deserves special attention due to their increased sensitivity to radiation. United Nations Scientific Committee on Effects of Atomic Radiation[1] has reported that early childhood exposure to ionizing produces a 2- to 3-fold more sensitivity than in adults.[1] This understanding has precipitated the establishment of guidance level or reference doses for pediatric patients undergoing diagnostic X-ray examinations, as it is a concern to various national and international organizations involved in radiation measurement, monitoring, and safety. It is therefore important that radiation dose to children arising from diagnostic medical exposure is minimized, due to their rapidly dividing cells and longer life expectancy.[2] Despite the advent of new imaging modalities such as ultrasound, computed tomography, and magnetic resonance imaging, the plain chest radiography remains the mainstay of pediatric chest imaging.[3]
Pediatric imaging is quite challenging for radiographers due to their smaller size, positioning difficulties, and vulnerable nature to radiation damage. Hence, certain skills, careful techniques, and a good understanding of their anatomy and psychology are critical to optimizing practice and reducing radiation burden during pediatric imaging.[4,5] Technically, pediatric chest radiography differs from an adult’s, as their small-sized chest, faster respiratory rate, and difficulty in observing required respiratory maneuvers are taken into consideration to adapt chest radiography to obtain diagnostically acceptable image quality, at a significantly reduced radiation dose.[5] As a result, very fast screens, short exposure time, and maximum source-to-image distance (SID) are used to improve imaging and reduce unsharpness due to movement or respiratory blur. Furthermore, careful collimation of the X-ray beam to the area of interest is applied. In addition to that, the radiographer must be aware of the radiation exposure to the gonad of the child and a lead strip must be placed over the gonadal area.[6] Overall, about 9.07% of the total number of pediatric chest radiographs consists of a non-thoracic structure resulting in radiation exposure to these areas, the radiation exposure to these structures increases as the patient decreases.[7] There is no gainsaying that there is a risk involved in every X-ray examination in pediatric patients.[6] There is therefore a need to optimize pediatric chest radiography, as it is one of the most common in pediatric imaging.
This study sought to investigate radiation equivalent doses during pediatric chest examinations.
MATERIAL AND METHODS
This study adopted a prospective and cross-sectional research design and was conducted between April 26 and July 2, 2021, at the University of Calabar Teaching Hospital, Calabar, Cross river state, Nigeria. Approval was sought from the Department of Radiography and Radiological science, University of Calabar, Calabar. A total of 85 pediatric patients (both males and females) aged 0–15 years, referred for chest X-ray examination in this facility (hospital), were recruited into the study. The chest radiography was taken for each child in erect and supine positions using the erect/table bucky. The head was kept straight and chin raised out of the field of view. The shoulders rolled anteriorly to throw off both scapulae from the lungs fields. A horizontal beam was centered to the seventh thoracic vertebra, which corresponds to the inferior angle of the scapulae. X-ray beam was collimated to include C7/T1 vertebrae, just inferior to the thoracolumbar junction, lateral to the skin margins. Children, who needed some form of immobilization, were immobilized and respiration (breathing) was observed to take exposures at end-expiration. Exposure factors used ranged between 40 and 80 kVp, 1–2 mAs, SID; 110 cm. No grid was used.
Patient demographics and chest X-ray exposure factors for each exposure were recorded using a spreadsheet. The equivalent dose for each chest radiography was calculated using the NUTECHRX software version. Synthesized data were analyzed using a pie chart for gender distribution of the pediatric patients and a bar chart to represent age groupings. Mean and standard deviation was calculated for the weight of pediatrics, age, kVp, mAs, and equivalent dose. Pearsonp, mAss. Mean and standard deviademonstrate the relationship between equivalent dose and other variables (weight, kVp, and mAs). All statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS) version 21.0. Statistical significance was set at P < 0.05.
RESULTS
The proportion of females in the study was 55% (n = 47), while the male accounted for 45%, (n = 38) of the total number of children [Figure 1]. About 60 of the patients in the study were between 0 and 5 years of age, while the group with the smallest number was aged 10 and above [Figure 2]. The estimated mean equivalent dose was 0.0046 ± 0.0026 mSv, while the mean of weight (kg), kVp, and mAs were 15.04 ± 14.51 kg, 58.28 ± 10.58V, and 1.79 ± 1.56 mAs, respectively [Table 1]. Mean equivalent dose was 0.00447mSv (uncertainty 0.0027) for female and 0.00464mSv (uncertainty 0.0026) for male, with no significance difference between them [Table 2]. (Mean plot) shows the mean values of Equivalent dose by age group. No difference exists in equivalent dose across the age grouping (P > 0.05) (one-way ANOVA) [Figure 3]. The mAs showed strong positive correlation with equivalent dose (r = 0.71, P = 0.05), while weight demonstrated a strong negative correlation with equivalent dose (r = −0.98, P = 0.05). The kVp indicated no statistical correlation with equivalent dose (P > 0.05) [Table 3].

- The frequency and percentage distribution according to gender.
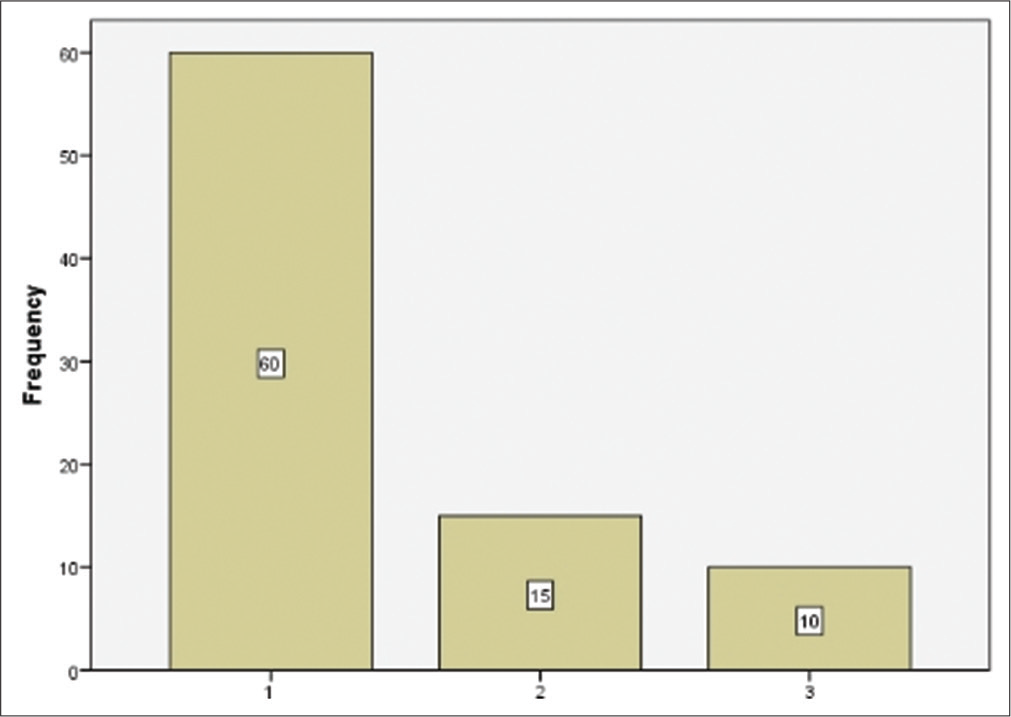
- Age grouping of pediatric patients for chest examination.
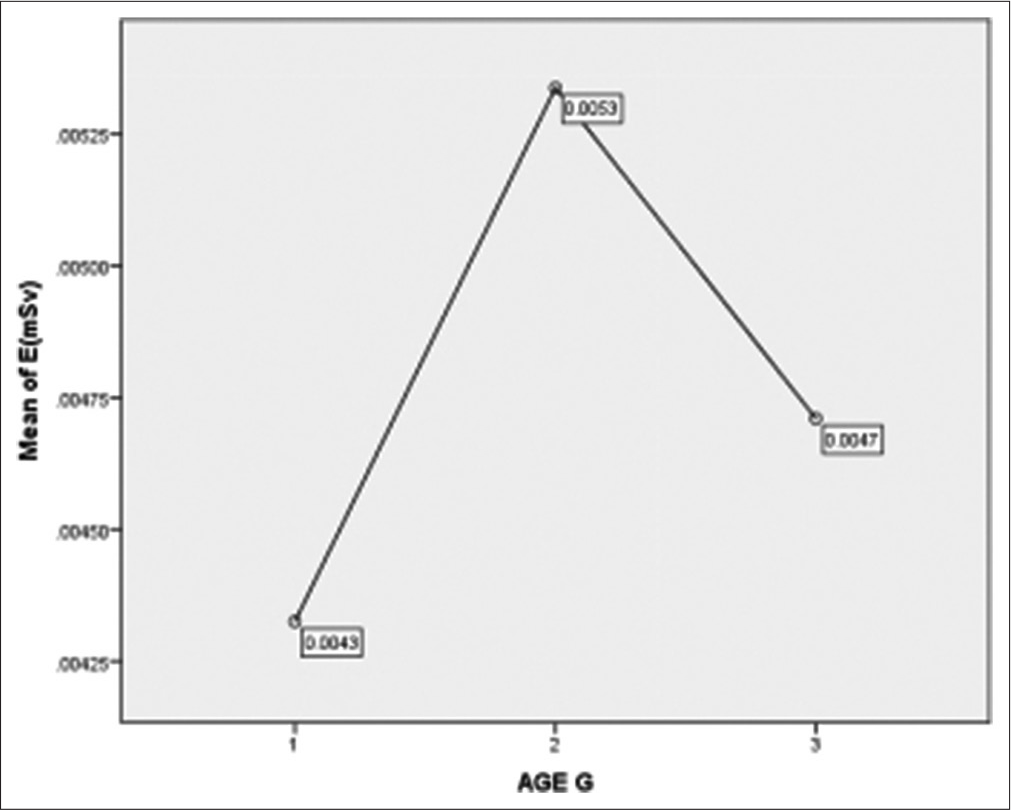
- (Mean plot) shows the mean values of equivalent doses by age group. No difference exists in equivalent dose across the age grouping (P > 0.05) (one-way ANOVA).
| N | Range | Minimum | Maximum | Mean | |
|---|---|---|---|---|---|
| Eq Dose | 85 | 0.0087 | 0.00100 | 0.00970 | 0.0046±0.0026 |
| Weight | 85 | 64.2 | 2.8 | 67.0 | 15.04±14.51 |
| (kg) | |||||
| kVp (v) | 85 | 44.0 | 40.0 | 84.0 | 58.28±10.58 |
| mAs (A) | 85 | 7.88 | 0.12 | 8.00 | 1.79±1.56 |
EqDose: Equivalent dose
| Correlations | R | P-value |
|---|---|---|
| EqDose* mAs | 0.71 | 0.05** |
| EqDose* kV | −0.035 | 0.0749 |
| Eqdose* Weight | −0.98 | 0.0370 ** |
| Equivalent dose between male and female | |||||
|---|---|---|---|---|---|
| Gender | n | Mean | t | P-value | |
| EqDose (mSv) | F | 55% | 0.00447±0.0027 | 2.96 | 0.768 |
| M | 45% | 0.00464±0.0026 | |||
EqDose: Equivalent dose
DISCUSSION
The equivalent dose quantity represents the stochastic health effect of low-level ionizing radiation on the human body and the probability of radiation-induced cancer and genetic damage. It is a concept employed for radiation protection as it attempts to measure the long-term biological consequence of a given exposure to radiation expressed in millisievert (mSv).
In this study, the mean equivalent dose to the pediatrics was comparable with results of similar research, and dose measurements were statistically the same across age grouping, in contrast to the findings of Ward et al.[8] and Roya et al.[9] In their study, a substantial difference in radiation dose across age groupings was reported, and this difference between the aforementioned study and the present study may be underlain by factors such as sample size, X-ray unit, and characteristics. In addition, Asoqwaetal et al.[10] in his study noted that SID and field size could have a significant effect on entrance skin dose and equivalent dose.
A similar result in terms of equivalent dose measurements was obtained by comparing equivalent doses between males and females, and this was in consonance with a related study by Alatts et al.[2]and Roya et al.[9] In their study on entrance skin dose, they found no statistical difference in the mean doses for both male and female gender. This could imply that the equivalent dose from X-ray may not be dependent on tissue gender-specific factors, but rather a function of absorbed dose and the radiation weighting factor for each type of radiation.[11]
The equivalent dose to the pediatric was seen to increase with the current-time product (mAs), and decrease with the child’s body weight. This implies a higher radiation requivalent dose to children with smaller weights, especially at higher mAs. Alatts et al.[2] report a similar outcome in the relationship between mAs and equivalent dose, while a contrary yield to the result of Bagherzadeh et al.[12] was observed between weight and equivalent dose in the present study. Since pediatrics have very high chances of cancer induction in the future from early radiation exposure, it is important for facilities to adopt measures to curtail unnecessary radiation exposure during pediatric radiography. Besides controlling exposure setting like mAs, a child’s weight could be factored into dose-limiting protocols in chest radiography to reduce undue exposures.
The mAs and pediatric weight are important determining factors of the equivalent dose during pediatric chest radiography and could be adapted to optimize practice, improve diagnostic yield, and reduce the dose to the pediatrics during pediatric chest radiography. The limitations of this study are the absence of exposure index (EI), which is a current metric for determining the level of exposure from a given radiographic investigation, particularly, the extrapolation of radiation dose from EI during exposure and the provision of the reference range and benchmark by which facilities can depend on for optimization of pediatric chest radiography and dose mitigation.
Recommendation
There is a need for facilities to adapt pediatrics-specific protocol based on a child’s weight in combination with mAs to improve practice in pediatric chest radiography.
CONCLUSION
The current-time product (mAs) and the weight of the child affect the equivalent doses for pediatrics during chest examinations. The weight of a pediatric in combination with the current-time product (mAs) could be useful in establishing a weight-specific protocol for pediatric chest radiography to control and optimize radiation dose and image quality.
Declaration of patient consent
Patient’s consent not required as patient’s identity is not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Sources and Effects of Ionizing Radiation United Nations, New York: Report to the General Assembly with Scientific Annex; 2000.
- [Google Scholar]
- Radiation doses from chest X-ray examinations for pediatrics in some hospitals of Khartoum state. Sudan Med Monit. 2013;8:186-8.
- [CrossRef] [Google Scholar]
- Radiographic Imaging and Exposure (6th ed). London: Elsevier Mosby; 2020. p. :65-71.
- [Google Scholar]
- Clark's Positioning in Radiography. (13th ed). Boca Raton, FL: CRC Press; 2016. p. :371-98.
- [CrossRef] [Google Scholar]
- Patternry in Diagnostic Radiology Vienna: International Atomic Energy Agency; 2007. p. :457.
- [Google Scholar]
- Radiation dose from common radiological investigations and cumulative exposure in children with cystic fibrosis: An observational study from a single UK center. BMJ Open. 2017;7:e017548.
- [CrossRef] [PubMed] [Google Scholar]
- Entrance skin dose measurements in paediatric chest x-ray. J Radiat Nuclear Med. 2020;1:23-8.
- [CrossRef] [Google Scholar]
- Assessment of radiation dose to paediatric patients during routine digital chest x-ray procedure in a government medical centre in Asaba, Nigeria. Med Sci Discov. 2021;8:155-60.
- [CrossRef] [Google Scholar]
- The 2007 recommendations of the internal commission on radiation protection. ICRP Publication 103. Ann ICRP. 2007;37:1-332.
- [CrossRef] [Google Scholar]
- Estimation of lifetime attributed risks (LARs) of cancer associated with abdominopelvic radiotherapy treatment planning (CT) simulations. Int J Radiat Biol. 2018;94:454-61.
- [CrossRef] [PubMed] [Google Scholar]




