
Translate this page into:
Radiographic assessment of the cardiothoracic ratio in the pediatric age group at a tertiary institution in North-Central Nigeria

-
Received: ,
Accepted: ,
How to cite this article: Chia MD, Mohammad H, Annongu TI, Abah OR, Abdallah R, Abdullahi A, et al. Radiographic assessment of the cardiothoracic ratio in the pediatric age group at a tertiary institution in North-Central Nigeria. Calabar J Health Sci 2022;6:65-71.
Abstract
Objectives:
The most common method for detecting cardiomegaly and calculating the cardiothoracic ratio (CTR) is through the use of chest radiography. Since 1919, when the CTR was first described, there has been an interest in its utility as a predicator of heart size, leading to a lot of research, notably in the adult Caucasian population. However, in the African pediatric age group, there is paucity of data on this subject. We aim to establish normative data on CTR and its determinants in Nigerian children aged 1–15 years, using chest radiographs.
Material and Methods:
This was a 7-month observational analytical study assessing chest radiographs of healthy children aged 1–15 years at the Radiology Department of Benue State University Teaching Hospital, Makurdi, from May to November 2021. The respondents’ biometrics and chest radiographs were obtained after the protocol was authorized by the institutional Health Research Ethics Committee. The CTR was calculated using measurements of the maximum transverse cardiac diameter (MTCD) and the maximum internal thoracic width (MITW). The data obtained were analyzed using Statistical Package for the Social Sciences version 26, and Microsoft Excel 2017. The statistical significance level was selected at P ≤ 0.05.
Results:
A total of 150 pediatric chest radiographs were evaluated, with a male: female ratio of 1.4:1. The study population’s mean age was 6.9 ± 4.8 years. There was a steady decrease in CTR with increasing age across the sexes. The mean CTR of the general population was 49.3%. Weight, height, age, and MITW correlated negatively but statistically significantly with CTR (P = 0.000), while the correlation of CTR with race, MTCD, and sex was not statistically significant (P = 0.657, 0.688, and 0.692, consecutively).
Conclusion:
The result of the study has established 49.3% as the mean CTR value of the pediatric age group in our environment. We also found out that CTR was significantly influenced by weight, height, age, and thoracic size (MITW).
Keywords
Cardiothoracic ratio
Maximum transverse cardiac diameter
Maximum internal thoracic width
Nigeria
Pediatric age (0–˂18 years)

INTRODUCTION
The cardiothoracic ratio (CTR) is a standard parameter for evaluating the cardiac silhouette.[1,2] The procedure is simple, inexpensive, widely available, and an excellent predictor of coronary heart disease mortality. It can be used to screen individuals with cardiomegaly and cardiovascular diseases using a single frontal radiograph.[3-5]
With a population of over 1 billion people, Africa plays a significant role in the global burden of cardiovascular diseases,[6] which are the primary causes of disability and premature mortality, especially in Nigeria.[7,8]
More sensitive modalities, such as echocardiography (ECG), computed tomography (CT), and magnetic resonance imaging, can be used to assess cardiac size. However, they are more expensive and not always readily available. In addition, both image acquisition and interpretation require specialist training.[9] Furthermore, CT is associated with a high risk of radiation exposure, making it unsuitable for routine CTR assessment.[10]
According to previous reports,[11-13] a CTR value of 60% is acceptable as the upper limit of normal in newborns, while a CTR value of 45% is considered normal in older children and adolescents.[13] However, these figures are subject to debate because a variety of factors, including age, race, body posture, physique, respiratory phase, geographic location, and technical flaws in the technique, can all affect the CTR result.[14,15] This is further compounded in the pediatric age group, especially in the 1st year of life, by a CTR, which is larger due to the more transverse heart position in the chest at that age compared to older children, thus creating a broad spectrum of normal values with normal growth and development.[16]
Anteroposterior (AP) chest radiographs are the gold standard for CTR evaluation in children younger than 5 years.[17] The drawback to this projection is an increased radiation dose to radiosensitive organs and magnification of the heart and mediastinum.[18] The posteroanterior (PA) views are performed on older children, who can obey instructions. In addition to less magnification of the heart, greater improvement in lung visibility, and diaphragm position, this projection offers a more stable position for these children because they can hold on to the unit, thereby reducing motion blur. In addition, the compression of breast tissue against the film cassette minimizes the density of tissues at the centering point bases, allowing for better visualization of the mediastinal structures. Moreover, because the X-ray beam transverses the patient’s chest from posterior to anterior, radiosensitive organs such as the thyroid, sternum, and developing breast receive less radiation dose.[19,20]
There is a paucity of literature on pediatric CTR in African and, by extension, Nigerian children. To the best of our knowledge, no such research has ever been conducted at Benue State University Teaching Hospital (BSUTH), Makurdi, our study area. The aim of this study is to establish normal data on CTR and its determinants using chest radiographs in Nigerian children aged 1–15 years.
MATERIAL AND METHODS
This was an observational and analytical study assessing 150 pediatric chest radiographs at the Radiology Department of BSUTH, Makurdi, from May to November 2021. This public teaching hospital serves as a referral center for the state in which it is located as well as other surrounding states in the country.
The inclusion criteria were healthy children aged 1–15 years who were brought by their parents or guardians for a pre-school medical examination and those who were referred or brought to have chest radiographs for reasons, other than cardiopulmonary diseases.
Based on the clinical history and physical examination, pediatric patients with symptoms of cardiomegaly, cardiopulmonary disease, or thoracic cage abnormality were excluded from the study. Those with foreign body aspiration or ingestion and with clinical or radiological features suggestive of chest infections were similarly excluded because of the role infections play as trigger factors in decompensated cardiac failure and, by extension, increased CTR. Inability to determine one or both heart borders on chest x-ray (CXR) also constituted an exclusion criterion.
Informed consent and assent were obtained from parents and guardians as well as the older children. Participation in the study was entirely voluntary, and all personal information was confidentially obtained. There was complete freedom to refuse consent or opt-out without repercussions. The participants’ weights and heights were obtained on a SECA electronic weighing scale (capacity 200 kg), model 769, made in Germany in 2007, and fitted with a stadiometer (height/length range of 200 cm). The weights of children below 5 years old were obtained by having their parents or guardians assist them onto the center of the weighing scale placed on a firm floor after removing heavy shoes, clothing, or hair ornaments. Those below 3 years were assisted to stay in a recumbent position for length measurements (cm) on the stadiometer. The older children were simply instructed to climb on the weighing scale, standing with both feet in the center of the scale for weight (kg) measurements, or to stand erect, feet flat, straight legs, arms by their side, and with leveled shoulders against the stadiometer for estimation of their height (cm), respectively.
A Daystar 5503 AGFA printer (Hamburg, Germany) in conjunction with a Philips medical system X-ray machine DNCGMBH-Roentgestrabe 24 D 22335 (Hamburg, Germany) with an AGFA medical system digitizer, equipment ID 10261788, was used for the radiographic examination.
The parents and guardians of participating children were asked to remove their wards’ clothing and jewelry from the waist up, particularly clothing with metal or shiny decorative materials, which are capable of affecting the diagnostic quality of the image. The patient’s plaited hair was untied before the patient’s positioning (supine or erect) for the two radiographic views (AP or PA).
For the AP chest projection, employed especially for children below 5, we used lead protective shielding aprons for the vital organs, the gonads, thyroid, and bowel which are close to the primary radiation beam. The head was maintained straight, the chin raised out of view, and the arms raised above the head to allow for the observation of the child’s breathing without much stress, ensuring at all times that the child was comfortably observing what was happening in the X-ray exposure room.[21]
The PA chest radiographs were performed for the older children who could obey instructions, with the shoulders touching the detector to ensure no rotation of the child. As they are located further away from the primary radiation beam, the radiosensitive organs receive a lower radiation dose. As such, this view is routinely preferred over the AP projection in diagnostic imaging in older children.[22]
Chest X-ray exposure was done in a full inspiratory effort to ensure that the 8–9th and 10th posterior ribs were visible in children aged 5 years or less and in the older children, respectively while watching the patient’s stomach to observe breathing movements. All radiographs were performed in the portrait orientation, with a well-collimated horizontal beam centered on the level of the 7th thoracic vertebra, approximately at the inferior angle of the scapula at a film focus distance of about 130 cm.
All children under the age of 5 were radiographed with an AP beam while lying supine on a towel-covered cassette. Uncooperative patients and those who could not obey instructions were diverted with toys, games, and/or child-appropriate language like “Stand still like a soldier” and “breathe in.”[20] A frequent strategy we employed was having a parent, guardian, or relative in the exposure room with the patient and holding them still. Only 3.0% of children needed blanket strap immobilizations. All children above the age of 5 who could obey instructions and cooperate were radiographed with a PA beam in an upright stance facing the detector. The AP supine projection is the best view in infants and young children by a factor of 2:1 because it offers the patient a more physiologic breathing position, making it convenient to obtain chest X-rays with more satisfactory inspiratory effort. When the infant is in this position, it is also easier to immobilize them. In addition, the smaller heart size at this age offsets any anticipated magnification due to the divergent beam.[17]
Technical quality was determined by a visual assessment of the film’s overall acceptability in terms of structural detail, based on adequate inspiratory effort, collimation, centering without rotation of the patient, and correct placement of side markers, as well as acceptable film contrast from adequate exposure/penetration by the X-ray beam.[17,23] Less than 5% of our exposures did not meet the standard criteria as outlined and had to be repeated.
The maximum transverse cardiac diameter (MTCD) and maximum internal thoracic width (MITW) were measured on viewing boxes with a transparent ruler under ideal viewing conditions, with their fluorescent tubes freshly replaced and viewing surfaces thoroughly cleaned, while minimizing excessive ambient lighting per the 1996 guidelines of the World Health Organization and Commission of European Communities.[24]
The horizontal distance between the most leftward and rightward borders of the heart as seen on the chest radiograph defined the MTCD, whereas the horizontal distance inside the rib cage at its widest point above the costophrenic angle defined the MITW [Figure 1]. These measurements were used to calculate the CTR as follows:
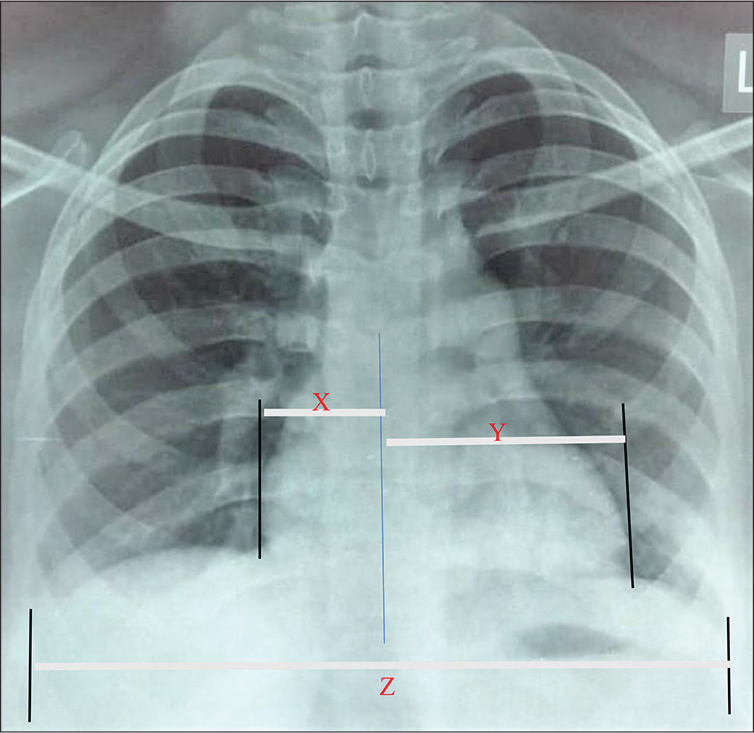
- A posteroanterior chest radiograph of a 14-year-old pediatric female patient depicts how to measure the maximum transverse cardiac diameter and maximum internal thoracic width. The cardiothoracic ratio is calculated as the ratio of these two measurements.
Where:
X (MRD) = Heart’s perpendicular most rightward diameter
Y (MLD) = Heart’s perpendicular most leftward diameter.
Z (ID) = Internal diameter of the chest at the level of the widest chest diameter
The data collected were analyzed and processed with the Statistical Package for the Social Sciences version 26 software and Microsoft Excel 2017. The significance criterion was chosen at P < 0.05. The results were presented using tables and figures. The protocols were approved by the institutional Health Research Ethics Committee.
RESULTS
One hundred and fifty pediatric chest radiographs were evaluated, out of which 88 (59.0%) were male and 62 (41.0%) were female as represented in [Figure 2]. Their age ranged from 1 to 15 years, with a mean and median age of 6.9 ± 4.8 and 6.0 years, respectively. At a 95% confidence interval for the mean, upper and lower bounds were 7.7 and 6.2, respectively, with an interquartile range of 8.00. The majority of the children 98 (65.0%) were between the ages of 6 and 10 years. This was followed by 33 (22.0%) children, in the age bracket of 1–5 years old, while the least number of children, 19 (13.0%), were those between the ages of 11 and 15 years as displayed in [Figure 3].
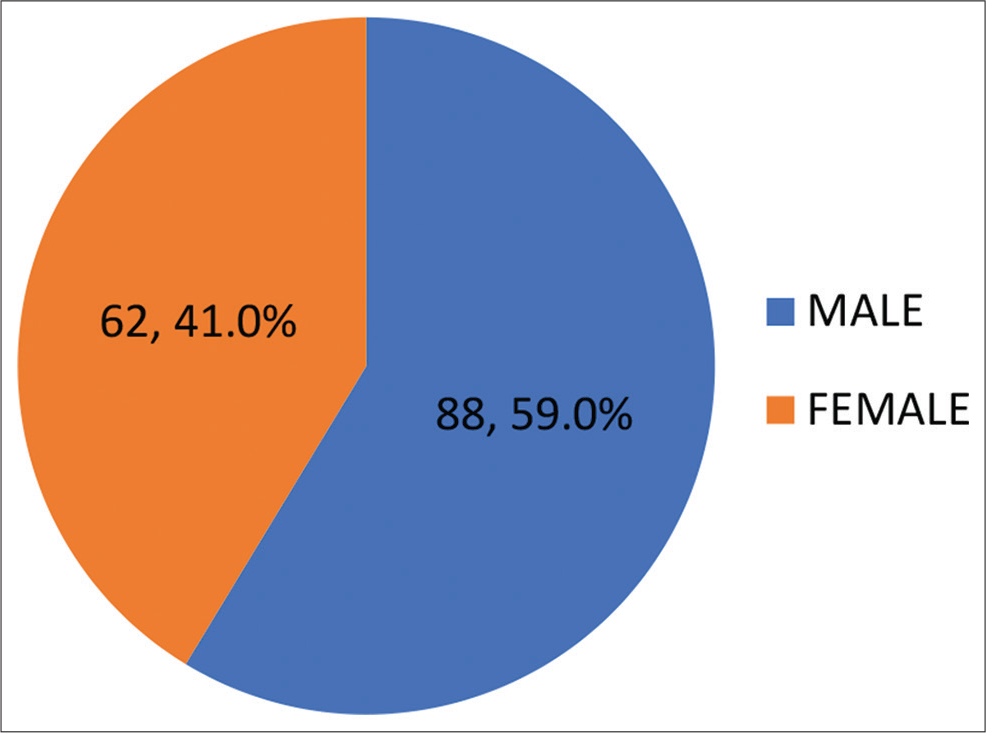
- Sex distribution of respondents.
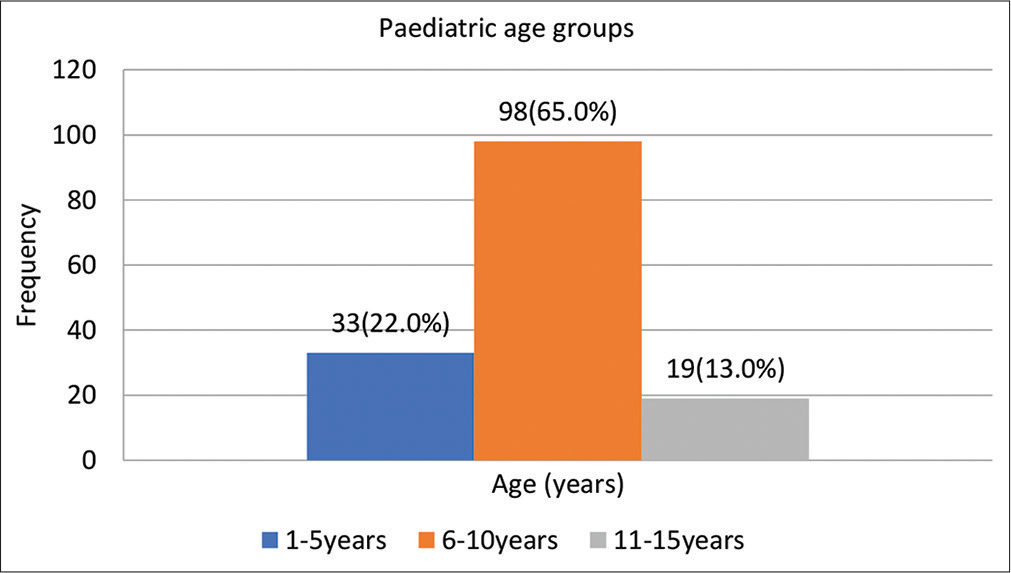
- Age group distribution of respondents.
[Table 1] illustrates the CTR across age groups and sexes. For males, females, and the general population of study, the mean CTR at 95% confidence interval was 49.2% (SD = 0.050 and margin of error = 0.006), 49.4% (SD = 0.050 and margin of error = 0.006), and 49.3% (SD = 0.048 and margin of error = 0.004), respectively.
| Sex | Age (years) | Mean CTR | N | Std. deviation | Std. error of mean | C.I (95%) |
|---|---|---|---|---|---|---|
| M | 1–5 | 0.5039 | 22 | 0.04161 | 0.00981 | 0.504±0.009 |
| 6–10 | 0.4960 | 51 | 0.04993 | 0.00721 | 0.500±0.007 | |
| 11–15 | 0.4620 | 15 | 0.04632 | 0.01196 | 0.462±0.012 | |
| Total | 0.4915 | 88 | 0.04917 | 0.00546 | 0.492±0.005 | |
| F | 1–5 | 0.5007 | 11 | 0.04605 | 0.01189 | 0.501±0.012 |
| 6–10 | 0.4962 | 47 | 0.04607 | 0.00651 | 0.507±0.007 | |
| 11–15 | 0.4400 | 4 | 0.03464 | 0.01732 | 0.440±0.017 | |
| Total | 0.4939 | 62 | 0.04694 | 0.00565 | 0.499±0.007 | |
| ∑ (M+F) | 1–5 | 0.5024 | 33 | 0.04301 | 0.00749 | 0.502±0.007 |
| 6–10 | 0.4961 | 98 | 0.04775 | 0.00485 | 0.500±0.005 | |
| 11–15 | 0.4574 | 19 | 0.04420 | 0.01014 | 0.460±0.010 | |
| Total | 0.4926 | 150 | 0.04801 | 0.00392 | 0.495±0.004 |
CTR: Cardiothoracic ratio
The sex distribution with mean MTCD, MITW, and CTR of the respondents is displayed in [Table 2]. The study population’s mean MTCD, MITW, and CTR are 24.27 cm, 33.72 cm, and 49.3% (range CTR = 37.0–64.0%), consecutively. There were sex variations in favor of males for both MTCD (M > F = 24.95 ± 13.69 > 23.14 ± 11.47) and MITW (M > F = 35.35 ± 22.59 > 31.02 ± 18.24) and also noted were a slight sex variation in favor of females for CTR (F > M = 0.494 ± 0.05 > 0.492 ± 0.05).
| N | MTCD | MITW | CTR (%) | |
|---|---|---|---|---|
| Sex | ||||
| Male | 88 | 24.95±13.69 | 35.35±22.59 | 0.492±0.049 |
| Female | 62 | 23.14±11.47 | 31.02±18.24 | 0.494±0.047 |
| Total | 150 | 24.27±12.88 | 33.72±21.69 | 0.493±0.048 |
| Minimum | 1 | 1 | 0.370 | |
| Maximum | 49 | 73 | 0.640 |
MTCD: Maximum transverse cardiac diameter, MITW: Maximum internal thoracic width, CTR: Cardiothoracic ratio
As shown in [Table 3], the MTCD and MITW values increased steadily with increasing age, even though not by the same proportion.
| AGE (years) | N | MTCD | MITW |
|---|---|---|---|
| 1–5 | 33 | 15.03±12.12 | 19.30±18.20 |
| 6–10 | 98 | 25.95±10.48 | 35.39±17.55 |
| 11–15 | 19 | 34.00±12.80 | 56.00±19.00 |
| Total | 150 | 24.27±12.88 | 33.72±21.69 |
MTCD: Maximum transverse cardiac diameter, MITW: Maximum internal thoracic width
The variables in this study are non-parametric because they did not match the normal distribution necessary for conducting Pearson’s (r) correlation, as such Spearman’s rank correlation (rs) was used as summed up in [Table 4]. Weight, height, age, and MITW were correlated negatively but statistically significantly with CTR (P =0.000), while the correlation with race, MTCD, and sex was statistically non-significant (P = 0.657, 0.688, and 0.692, consecutively).
| Variable | Spearman’s correlation (rs) | P value |
|---|---|---|
| Weight | −0.405 | 0.000 |
| Height | −0.367 | 0.000 |
| Age | −0.361 | 0.000 |
| MITW | −0.324 | 0.000 |
| Race | 0.037 | 0.657 |
| MTCD | 0.033 | 0.688 |
| Gender | −0.033 | 0.692 |
MTCD: Maximum transverse cardiac diameter, MITW: Maximum internal thoracic width, CTR: Cardiothoracic ratio
[Figure 4] depicts a scatter plot with a classical relationship, displayed by the dashed trendline, indicating that CTR decreases with increasing age and vice versa.
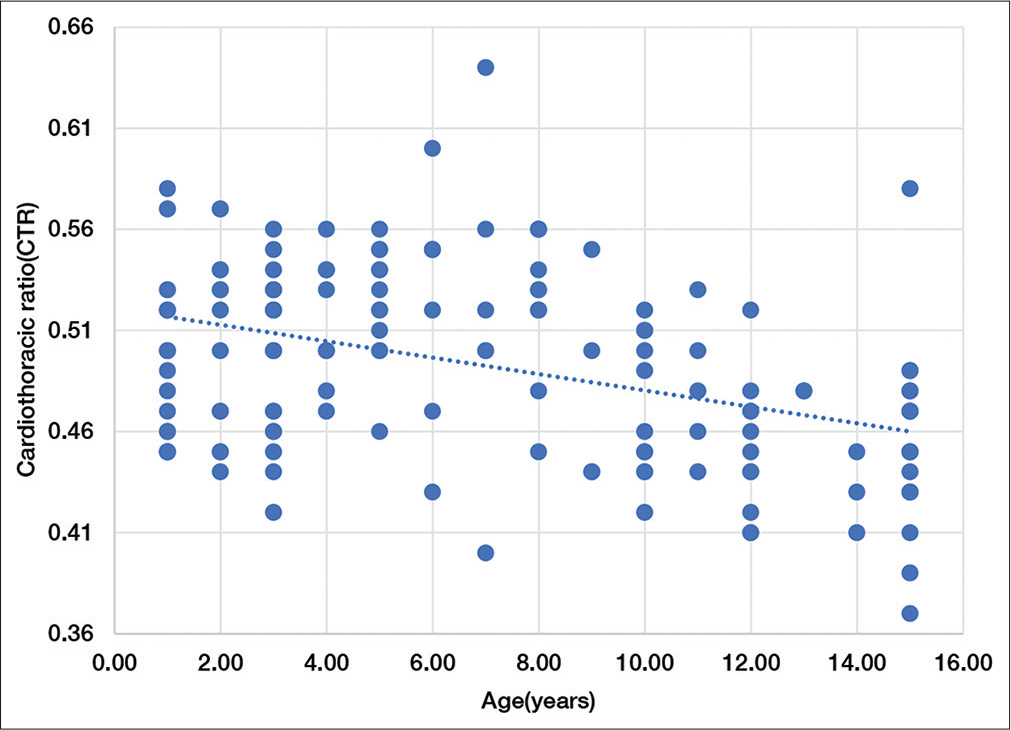
- Distribution of the association between CTR and AGE.
DISCUSSION
Our study showed a steady decrease in CTR with increasing age across sexes. The mean CTR of males, aged 1–5 years, 6–10 years, and 11–15 years, was 50.4%, 49.6%, and 46.2%, respectively, while similar age groups for females had a mean CTR of 50.1%, 49.6%, and 44.0%, respectively. This is because the cardiac silhouette is more transverse in early childhood, creating the false impression that the heart is larger in the formative years of life.[16,25] The statistically significant (P = 0.000) but negative correlation (rs = 0.361) between age and CTR in our study implies that as the age increases, the CTR decreases and vice versa.
Our CTR values were comparable but slightly higher than those of a study in Enugu by Obikili et al.,[14] which described the mean CTR values between sexes in the 5–9, 10–14, and 15–19 years age groups as 47.7%, 45.7%, and 44.1% for males and the corresponding values for females as 49.7%, 45.0%, and 45.1%, consecutively. Cowan[26] reported much lower mean CTR values across sexes on 9–14 years olds in Scotland in a similar study. The difference between our index CTR values and those from the previous research[14,26] could be explained by the fact that these authors used a slightly different methodology than we did, with their CTR values calculated using different pediatric age groups from different geographical locations as well as variations in radiographic techniques.
Despite the disparities in age groups, both our index study and that of Obikili et al.[14] reported that CTR was proportionally higher than that reported by Cowan[26] regardless of sex. This could just be a coincidence, although Africans have been said to have a smaller MITW and a relatively higher MTCD.[14] Inference to the computation of CTR as a ratio of MTCD over MITW could thus explain the greater CTR in Africans compared to Caucasians, because the CTR is bigger when the MTCD is higher and the MITW is smaller.
Our study reported a mean MTCD of 24.27 ± 12.88 and an MITW of 33.72 ± 21.69, respectively. Males had a slightly greater MTCD than females (M > F = 24.95 ± 13.69 > 23.14 ± 11.47). Differences in levels of physical activity and morphology (body size) among sexes may explain the sexual variation in MTCD.[15] Girls are disadvantaged and less favorably influenced by socioecological factors at the individual, family, school, and environmental levels, with the girls engaging in approximately 17% less total daily physical activity than boys.[27,28] The MTCD values in our research increased steadily with the advancing age of our respondents. The increase in MTCD values with age coincides with a period of rapid human growth hormone-triggered growth spurts, leading to rapid increases in heart size due to increased cardiac demands.[29] Our findings were largely in agreement with, but quantitatively higher than the MTCD values reported by an earlier study in 2010,[14] which used only PA chest radiographs in their assessment of MTCD values and included several pediatric age groups from 5 to 19 years old. We observed an almost similar trend with the MITW when compared with the same study[14] above. In our research, males also had a slightly greater MITW than females, with increasing values of MITW with age. Although thoracic size is influenced by age, gender, and race, the increase with age, in our research, is very important as it allows for more efficient pediatric thoracic expansion to compensate for the lesser efficiency of the diaphragms, decreased rib cage mobility, and compliance.[30,31]
Both the weight and height of children in our study correlated negatively but statistically significantly with CTR (P = 0.00). CTR, in our study, best correlated with weight (rs = 0.405), height (rs = 0.367), and then age (rs = 0.361) of the respondents. Although there was a paucity of data in the literature on the relationship between CTR and weight in children, weight-specific reference values are the best local recommended values to be used in the clinical evaluation of CTR, in our environment.
In a study in Spain, Escolar et al.[32] reported the role environmental factors, such as poor nutrition and infections, with influenza or pneumococcal agents, play in causing cardiac enlargement and, as a result, increased CTR. The participants in our index study were, however, healthy as required by the study’s inclusion criteria. The preposition that infections or malnutrition might be responsible for the larger CTR of Africans may not be, therefore, tenable in our study.
We hope that the findings of this study will have a substantial impact on the differing opinions on the utility of CTR as a traditional and well-known chest radiographic index of cardiac function, with capabilities for accurate diagnosis and management of cardiovascular diseases.
CONCLUSION
We have established 49.3% as the mean CTR value in the pediatric age group in our environment. The research presented MITW as a better index of CTR than MTCD. Weight was likewise found to be a good predictor of CTR, followed by height, then age.
When actual local values are unknown, relying on imported CTR values, especially for referencing, can result in a cascade of undesirable consequences, including delayed or unjustified diagnosis and treatment, wrong prescription dosage, and needless medicaments.
We are optimistic that the results from our index study will not only have a compelling effect on the divergent views on the importance of CTR but also highlight the usefulness of this simple measurement in epidemiology and pediatric clinical practice.
Acknowledgment
We sincerely thank the parents and guardians of all the respondents for their kind permission to allow their wards to participate in the study. We are also indebted to the management of the BSUTH, Makurdi, where the study was conducted, and in particular, the radiography unit, for their kind permission in allowing us to make use of their center for data collection.
Recommendations
In pediatric chest imaging, healthcare providers have a key role to play in deciding whether a radiographic examination is justifiable or not. It is, therefore, recommended that they must also recognize the benefits as well as the risks of these examinations, which are small but real.
It cannot be overemphasized how important it is for a pediatrician to confer with a radiologist when requesting a chest X-ray for a child. However, the radiologist is also obliged to do only those examinations for which the benefits far outweigh the risks, as well as develop protocols and adapt imaging procedures to suit the unique needs of the pediatric patient. Any questions posed by either side should initiate a healthy discussion aimed at improving the child’s care in a mutually beneficial manner.
Limitations of the study
There are inherent challenges in the radiographic imaging of the pediatric chest, such as choosing a child-appropriate language for instruction, professional training of personnel in the skills of communication with the child, difficulty in achieving good inspiration, and the need to minimize radiation dose, and the likelihood of motion blur. In addition, the sample size of the study was relatively small, which makes the findings less generalizable in our context. All of these constituted limitations to the study, including the fact that we did not use any light procedural sedation to calm apprehensive children to control excessive movement to limit image degradation, nor did we use ECG to assess cardiomegaly and exclude structural abnormalities. As such, caution should be exercised when interpreting the findings, as they may not be representative of all Nigerian children aged 1–15 years.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- A quantitative evaluation of heart size measurements from chest roentgenograms. Circulation. 1973;47:1289-96.
- [CrossRef] [PubMed] [Google Scholar]
- Cardiothoracic ratio and body habitus in a Nigerian population. Biomed Res. 2007;18:119-22.
- [Google Scholar]
- Cardiothoracic ratio and relative heart volume as predictors of coronary heart disease mortality. The Whitehall study 25-year follow-up. Eur Heart J. 1998;19:859-69.
- [CrossRef] [PubMed] [Google Scholar]
- The cardiothoracic ratio in newborn infants. AJR Am J Roentgenol. 1981;136:907-13.
- [CrossRef] [PubMed] [Google Scholar]
- Radiographic determination of cardiomegaly using cardiothoracic ratio and transverse cardiac diameter: Can one size fit all? Part one. Pan Afr Med J. 2017;27:201.
- [CrossRef] [PubMed] [Google Scholar]
- Cardiovascular disease in Africa: Epidemiological profile and challenges. Nat Rev Cardiol. 2017;14:273-93.
- [CrossRef] [PubMed] [Google Scholar]
- Cardiovascular disease and its determinants: Public health issue. J Clin Med Ther. 2016;1:1-5.
- [Google Scholar]
- WHO and Nigerian Government Move to Curb Cardiovascular Diseases Geneva: World Health Organization. 2019. Available from: https://www.afro.who.int/news/who-and-nigerian-government-move-curb-cardiovascular-diseases [Last accessed on 2021 Jul 14]
- [Google Scholar]
- Cardiothoracic ratio and body mass index in normal young adult Nigerians. J Med Trop. 2014;16:47-51.
- [CrossRef] [Google Scholar]
- Radiation risk to children from computed tomography. Pediatrics. 2007;120:677-82.
- [CrossRef] [PubMed] [Google Scholar]
- Roentgen evaluation of cardiomegaly in the newborn period and early infancy. Pediatr Clin North Am. 1971;18:1031-58.
- [CrossRef] [PubMed] [Google Scholar]
- The Neonatal and Paediatric Chest. Available from: https://radiologykey.com/the-neonatal-and-paediatric-chest [Last accessed on 2022 May 18]
- [Google Scholar]
- Determination of standard reference cardiothoracic ratio and the relationship with body parameters as a patient's health indicator for clinical application. Int J Sci Res Sci Eng Technol. 2019;6:318-26.
- [CrossRef] [Google Scholar]
- Aortic and heart dimensions of children and adolescents in a Nigerian population. Biomed Res. 2010;21:195-8.
- [Google Scholar]
- Evaluation of cardiothoracic ratio of normal subjects in Al Madinah Al Munawwara using chest radiographs. Pensee J. 2014;76:374-85.
- [Google Scholar]
- Available from: https://www.ohsu.edu/school-of-medicine/diagnostic-radiology/pediatric-radiology-normal-measurements [Last accessed on 2021 Mar 26]
- Comparison of AP supine vs PA upright methods of chest roentgenography in infants and young children. J Natl Med Assoc. 1984;76:171-5.
- [Google Scholar]
- Establishing the cardiothoracic ratio of non-hypertensive patients using posteroanterior (PA) chest radiographs in an indigenous Nigerian population. J Med Sci Clin Res. 2021;9:1-9.
- [Google Scholar]
- Pattern of radiographic findings in pediatric chest radiographs in Enugu state, Nigeria: Multi-center study. J Biomed Sci. 2019;8:14.
- [Google Scholar]
- Chest Radiograph (Paediatric) Available from: https://radiopaedia.org/chest-radiograph-paediatric [Last assessed on 2021 Mar 26]
- [Google Scholar]
- Paediatric Chest (AP Erect View) Available from: https://radiopaedia.org/articles/paediatric-chest-ap-erect-view?Lang=us [Last accessed 2021 Mar 26]
- [Google Scholar]
- Paediatric Chest (PA Erect View) Available from: https://radiopaedia.org/articles/pediatric-chest-pa-erect-view?Lang=us [Last accessed on 2021 Mar 26]
- [Google Scholar]
- The normal chest: Methods of investigation and differential diagnosis In: Sutton D, ed. Textbook of Radiology and Imaging (7th ed). Edinburg, UK: Elsevier; 2003. p. :5.
- [Google Scholar]
- Viewing conditions for diagnostic images in three major Dublin hospitals: A comparison with WHO and CEC recommendations. Br J Radiol. 2003;76:94-7.
- [CrossRef] [PubMed] [Google Scholar]
- Cardiothoracic ratio in Negroes in Southern Africa. Postgrad Med J. 1972;48:584-9.
- [CrossRef] [PubMed] [Google Scholar]
- The heart-lung coefficient and the transverse diameter of the heart. Br Heart J. 1964;26:116-20.
- [CrossRef] [PubMed] [Google Scholar]
- Why are girls less physically active than boys? Findings from the LOOK longitudinal study. PLoS One. 2016;11:e0150041.
- [CrossRef] [PubMed] [Google Scholar]
- Association of moderate to vigorous physical activity and sedentary time and cardiometabolic risk factors in children and adolescents. JAMA. 2012;307:704-12.
- [CrossRef] [PubMed] [Google Scholar]
- Growth of the heart related to bodily growth during childhood and adolescence. Pediatrics. 1948;2:382-404.
- [CrossRef] [PubMed] [Google Scholar]
- Establishing the cardiothoracic ratio using chest radiographs in an indigenous Ghanaian population: A simple tool for cardiomegaly screening. Ghana Med J. 2015;49:159-64.
- [CrossRef] [PubMed] [Google Scholar]
- Variations in dimensions and shape of thoracic cage with aging: An anatomical review. Anat J Afr. 2014;3:346-55.
- [Google Scholar]
- Impact of environmental factors on heart failure decompensations ESC Heart Failure. . 2019;6:1226-32.
- [CrossRef] [PubMed] [Google Scholar]




