
Translate this page into:
Laryngopyocele: 10 Years’ Experience in a Tertiary Institution, South-South, Nigeria


*Corresponding author: Abiola Grace Adekanye, Department of Otorhinolaryngology, University of Calabar, Calabar, Cross River, Nigeria. abiolaadekanye@gmail.com, abiola.adekanye@unical.edu.ng
-
Received: ,
Accepted: ,
How to cite this article: Adekanye AG, Ugbem TI, Kajogbola G, Umana AN. Laryngopyocele: 10 years’ experience in a tertiary institution, South-South, Nigeria. Calabar J Health Sci 2020;4(2):84-8.
Abstract
Laryngopyocele is an infected laryngocele: Rarer than laryngocele. An estimated 8% of laryngoceles get infected and become laryngopyocele with features of acute airway obstruction and sepsis with resultant fatality. Laryngocele is more common in Caucasian males population after the 5th decades of life. Mostly acquired though could be congenital. Most are unilateral with no predominance for the left or the right. Recently, laryngocele is categorized into internal or mixed (combined). Laryngopyocele accounted for 0.15% of 1376 ENT surgical procedures done in our operative theatre in a period of 10 years. Both were males in their 3rd decade. The first case reported with clinical features of upper airway obstruction from left laryngopyocele. Plain radiographs and computed scan of the neck revealed features of right laryngocele with contralateral left laryngopyocele. The second patient had recurrent right laryngopyocele. Twice general practitioners previously operated upon him before presenting in our facility. The two cases were successfully managed through external approach under general anesthesia with a small size endotracheal intubation. The mean follow-up period was 4 years without recurrence. There is dearth of literature on this subject in our environment; therefore, this article is an addition to literature.
Keywords
Laryngocele
Laryngomucocele
Laryngopyocele
Saccule
Recurrent

INTRODUCTION
Laryngocele is abnormal dilations of the laryngeal saccule filled with air and maintain a connection with the laryngeal lumen, if get infected it becomes laryngopyocele.[1,2] The exert etiopathogenesis of laryngocele could not be fully explained; however, both congenital and acquired factors are involved.[1] Laryngocele though is a benign disorder, it is important to rule out malignancy especially supraglottic cancer as an etiological factor.[1,3,4] Laryngoceles are classified into internal and combined according to their relationship with the thyrohyoid membrane. It was formally classified into internal, external, and mixed. However, this classification has been abandoned because purely external laryngoceles cannot exist as laryngoceles originate at laryngeal saccules.[2,4] Internal laryngoceles are confined within the larynx and dissect posterosuperiorly into the false vocal fold and aryepiglottic fold. The combined or mixed laryngoceles are those that extend upward and protrude through the thyrohyoid membrane to the neck.[2] Obstruction to the neck of laryngocele could lead to accumulation of mucus produced by mucous glands of the lining epithelium with resultant laryngomucocele and if infected it transformed into laryngopyocele.[1,2,5] This may therefore present with features of acute airway obstruction and sepsis with resultant fatal outcome.[5]
The majority of laryngocele may be completely asymptomatic especially if the lesion is small, however, symptoms varied according to the types. The internal variety may present with clinical features often caused by mass effect exerted by the laryngocele: Dysphonia, hoarseness, cough, sore throat, dysphagia, stridor, and even airway obstruction. On the other hand, the symptomatic combined laryngocele patients may experience hoarseness, inspiratory stridor, sore throat, cough, sudden neck mass, and acute respiratory distress.[4]
Radiologic studies are essential for determining the type, size, and extent of laryngocele, searching for associated malignancies as well as for planning the management.[4] The treatment of laryngoceles depends on clinical and radiological features. Patients with severe airway obstruction may need emergency tracheostomy to secure airway before definitive treatment is given.[2]
Our first case had left mixed laryngopyocele with contralateral right laryngocele of 18-year history of hoarseness that progressed to upper airway obstruction at presentation in our clinic, while the second patient had recurrent right combined laryngopyocele, which was preceded by neck mass that was excision twice by general practitioner. The management challenges encountered in the first case includes inability to clinically demarcate the left laryngopyocele from the right laryngocele, and disappearance of right laryngocele both on palpation and on direct laryngoscopy after excision of left laryngopyocele. However, the two cases were successfully managed through external approach and had median period of 4 years follow up without recurrence.
FIRST CASE STUDY
A 33-year-old male long distance driver, which presented with 18-year history of insidious, progressive and persistent hoarseness, snoring, and stator. Two years before presentation, he noticed painless left neck swelling, which later became painful with associated dyspnea, stridor, cough, and chest pain of 4-week duration. He was not a wind instrument player or glass blower, does not strain his voice, and was never a bus conductor. Patient used to smoke Indian hemp about 4 wraps a day and about 7 sticks of cigarette for over 4 years, but no history of injections on the neck. He also takes alcohol, about 4 bottles of beer daily and spirits, still taking alcohol. He had multiple sexual partners but no oral sex. He was treated with antibiotics and diclofenac before presentation.
Examination revealed a young man in mild respiratory distress with inspiratory stridor, RR 23C/Min but no cyanosis. There was a neck mass, extending from left to the right 1/3 of anterior triangle of the neck, soft and gurgling or hissing sound on compression and no differential warmth. Plain radiograph soft tissue neck and CT scan revealed right laryngocele and the left laryngopyocele [Figures 1 and 2]. Blood parameters were normal. Examination under anesthesia through direct laryngoscopy revealed left laryngopyocele [Figure 3a; Multimedia 1 (https://youtu.be/DFN9DY5Fp9A)]. Laryngopyocele was excised through external approach under general anesthesia with small size endotracheal intubation [Figure 3b]. Post-operative condition was satisfactory. Histology report confirmed laryngopyocele [Figure 4]. He has been following up for 1 year with significant reduction in size of right laryngocele and no recurrence on the left [Figure 5].
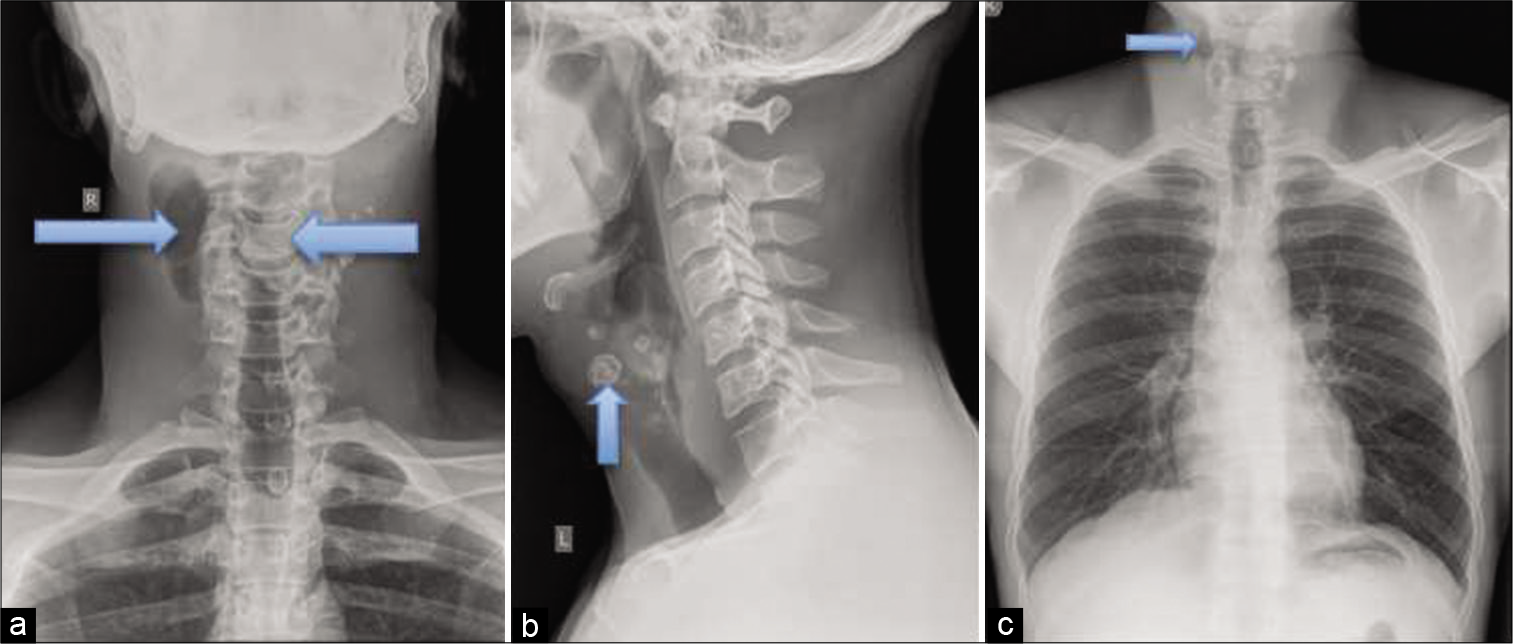
- A 33-year-old man with right laryngocele and left laryngopyocele presented with upper airway obstruction. Plain radiographs soft tissue neck: (a and b) AP and lateral views showing amorphous opacities of calcific density with the left anterolateral cervical soft tissue planes with well-defined lucencies on the right side (arrow). There is straightening of the normal cervical lordosis with preservation of the heights and alignments of the vertebral bodies as well as their densities. The intervening disc spaces, pedicles, and the posterior elements are preserved. (c) CXR showing that the heart, lung fields, and the overlying rib cage are within normal limits.
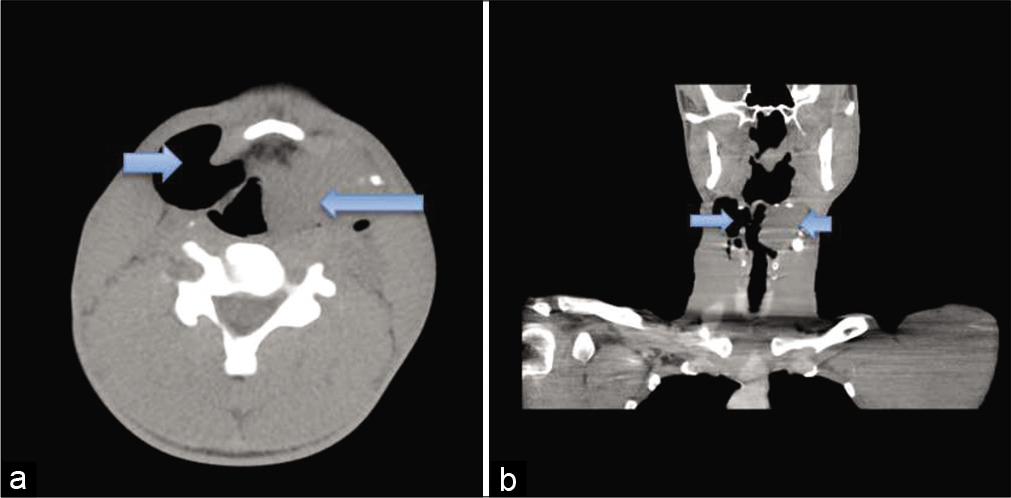
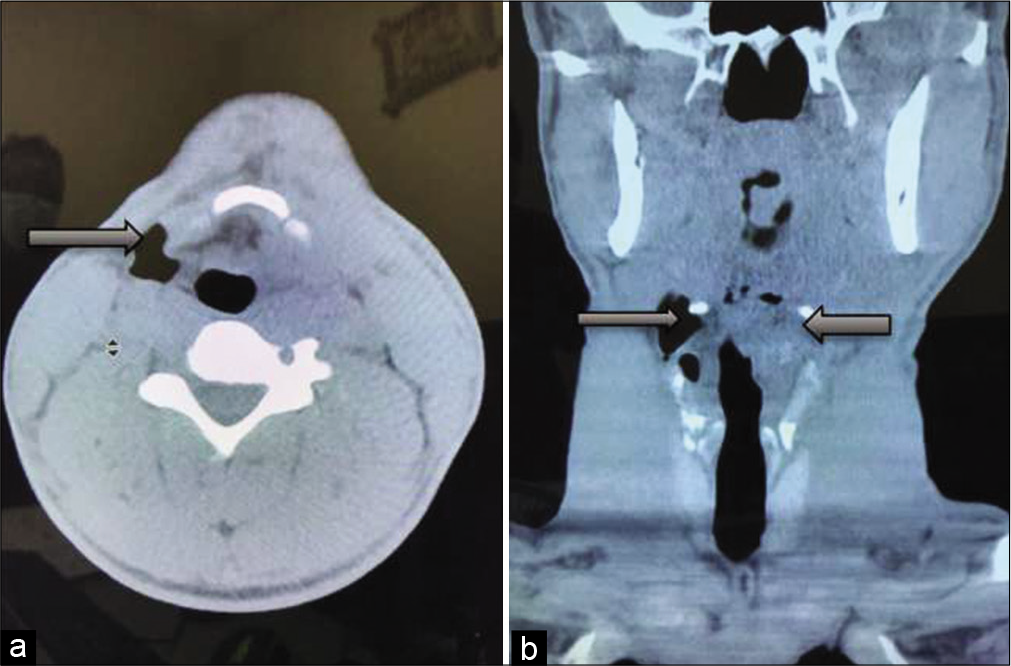
- A 33-year-old man with features of upper airway obstruction with significant left sided neck mass. Computed tomographic images (a) axial and (b) coronal views revealed an enhancing lobulated ovoid isodense mass, with peripheral amorphous calcifications (likely displaced laryngeal cartilages), arising from the left border of the laryngeal vestibule. Resultant asymmetry and narrowing of the adjacent airway noted. The mass measures 4.12 cm × 3.80 cm in its widest coronal dimensions. There is a well-defined air-dense collection contralateral to the aforementioned mass (blue arrows).
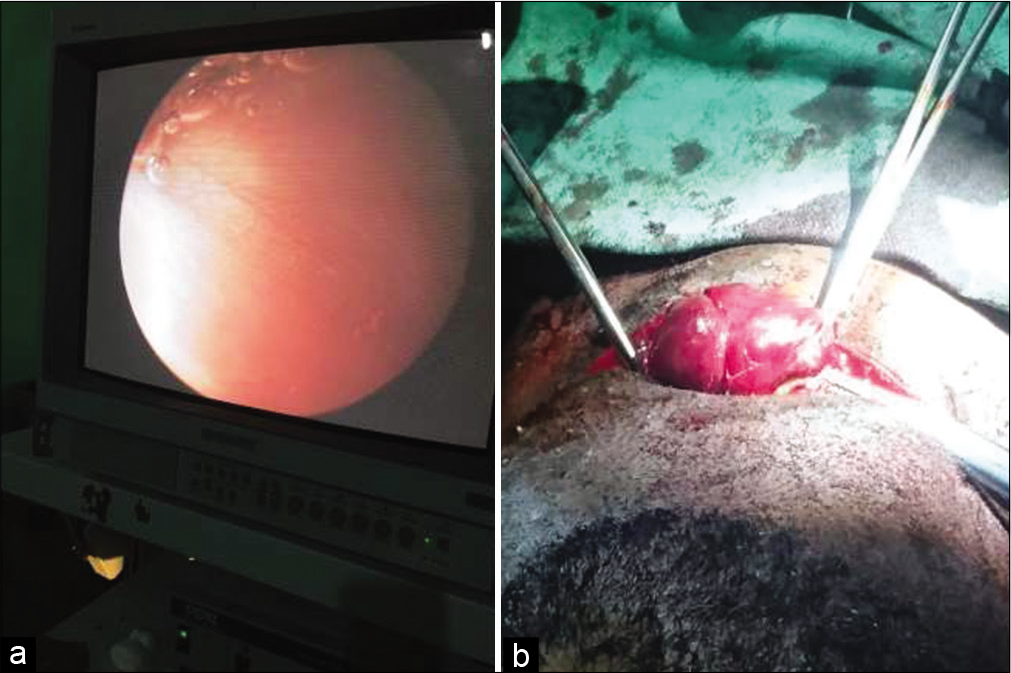
- (a) Internal component of left mixed laryngopyocele. (b) Left laryngopyocele being dissected out.
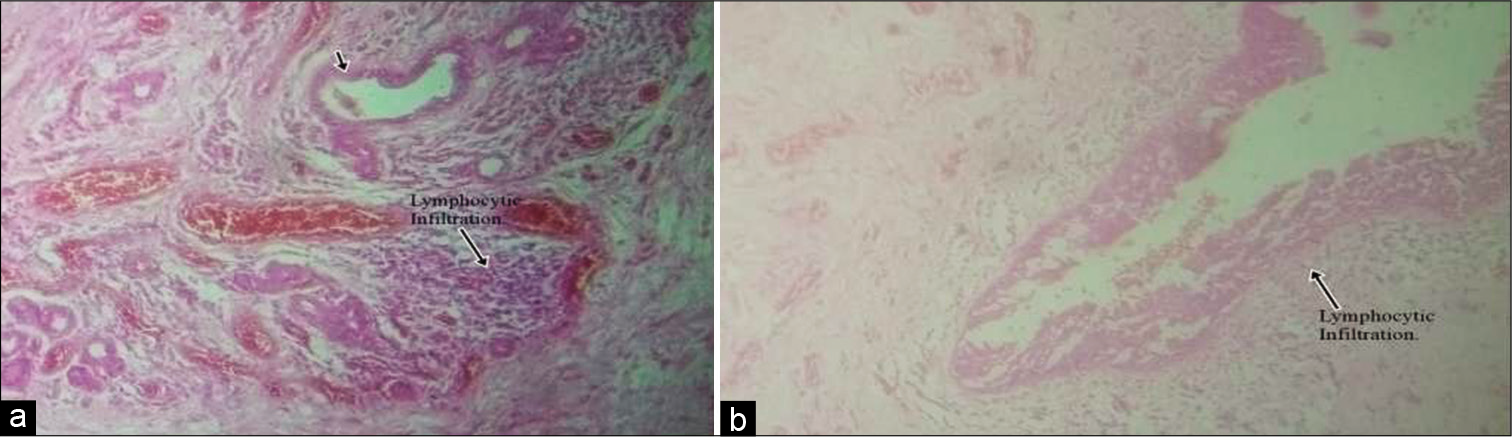
- Plate 1: H&E ×100: Photomicrograph shows a cyst wall lined by ciliated respiratory epithelial-lined cysts with lymphocytic infiltration (black arrow) consistent with a laryngopyocele. Plate 2: H&E ×400: Photomicrograph shows a cyst wall lined by ciliated respiratory epithelial-lined cysts with lymphocytic infiltration consistent with a laryngopyocele.
- Post-excision of left laryngopyocele of a 33-year-old man who presented with upper airway obstruction due to left laryngopyocele and laryngocele. Computed tomographic images: (a) Axial and (b) coronal after surgery showing significant reduction in the size of right laryngocele and complete resolution of left laryngopyocele (black arrows).
SECOND CASE
A 38-year-old undergraduate that presented himself to our clinic with 2 months history of recurrent right neck mass with associated hoarseness, blowing sound in the swelling during sleep, and dysphagia. However, no associated history of cough, chest pain or dyspnea. He had similar mass on the affected side of the neck 6 years before this particular onset following which he had operation done in two different occasions outside our health facility. Examination revealed a young man with obvious mass on right side of the neck; 12 by 7 cm in diameter with healed scar over it, not tender, fluctuant, and not attached to underling structure and he was not in respiratory distress. Blood parameters were within normal limits. CT scan showed a well-defined lobulated thin walled air-filled lesion in the right parapharyngeal space in continuity with the laryngeal ventricle and lateral to the thyrohyoid membrane.
The mass was excised through external approach under general anesthesia with endotracheal intubation and procedure was uneventful. Histologic report confirmed laryngopyocele. He was followed up for 7 years with no recurrence.
DISCUSSION
Laryngocele is a rare benign disease of the larynx occurring in about 1 per 2.5 million people annually in United Kingdom.[6] Laryngopyocele is an infected laryngocele, a very rare occurrence. An estimated 8% of laryngoceles get infected to become laryngopyocele1 with resultant vital emergency. Laryngocele affects males more than females at ratio of 5:1, with the peak incidence between 5th and 7th decade though it could be seen in any age. Most are unilateral with no predominance for the left or the right.[4] Out of 1376 ENT surgical procedures done in our theatre for the period of 10 years, only 2 cases (0.15%) of laryngopyocele were recorded in our operation register. Both were males, in their third decade and both had mixed laryngopyocele. In addition, one of the two cases had laryngocele on the contralateral side.
The etiology of laryngocele is unknown; however, the main associated factors leading to its formation include congenital predisposition, increase intralaryngeal pressure, and weakness of the laryngeal tissues.[7] Laryngocele may be either completely asymptomatic if the lesion is small or symptomatic with clinical features of acute upper airway obstruction.[4,8] The cause of this disease in two cases was probably due congenital disposition in the absence of history of raised intralaryngeal pressure. The first case had been hoarseness since he was a teenager. He reported for treatment 18 years after the onset of the disease with signs and symptoms of upper airway obstruction. The second case had sudden neck mass without respiratory distress at age of 32 years.
The diagnosis of laryngocele is confirmed by radiological investigation, surgical exploration, resection, and pathological examination.[4,9]
There is no consensus regarding surgical treatment though the external approach is still preferred by most surgeons.[2,9] Endoscopic management has gained popularity in the last 2 decades following advent of microlaryngoscopic surgery and CO2 lasers.[2,10] However, the systematic review by Al-Yahya et al. recorded 10 of 18 patients operated through external approach had tracheostomy done.[1]
The two patients had direct laryngoscopy examination of the larynx, excision through external approach without pre- or post-operative tracheostomy. The operations were uneventful and histologic report confirmed laryngopyocele. The management challenge we encountered was that the laryngocele on the right side of our first case became nonvisible through direct laryngoscopy after excision of the left laryngopyocele. Furthermore, the crepitus palpated on the right side of the neck was completely resolved. However, post-operative CT scan of neck revealed significant reduction on the right laryngocele and complete resolution of left laryngopyocele.
CONCLUSION
External approach for excision of laryngocele or laryngopyocele is still useful, especially in medical centers where facility for microlaryngoscopic surgery and CO2 lasers cannot be accessed. We advocate prompt referral of cases of this nature by general practitioners to otolaryngologists for proper evaluation and management to prevent complications and recurrence from inappropriate procedures. The two cases were successfully managed with no recurrence. This article is an addition to body of literature because, to the best knowledge of the authors, there is scarcity of publication on laryngocele/laryngopyoce from our center.
Acknowledgment
The authors acknowledged the nurses, medical record staff, and other health workers that took part in the management of these patients.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Videos available on:
VIDEO
Multimedia 1: Laryngoscopic review of laryngopyocele. Video is accessible from the portal.
References
- Laryngopyocele: Report of a rare case and systematic review. Ann Saudi Med. 2016;36:292-7.
- [CrossRef] [PubMed] [Google Scholar]
- Treatment of laryngoceles: What is the progress over the last two decades? Biomed Res Int. 2014;2014:819453.
- [CrossRef] [PubMed] [Google Scholar]
- Laryngopyocele: Presenting with pressure symptom. Int J Appl Basic Med Res. 2015;5:228-30.
- [CrossRef] [PubMed] [Google Scholar]
- Bilateral laryngocele causing epiglottic deformity and upper airway obstruction. Turk Arch Otorhinolaryngol. 2019;57:99-101.
- [CrossRef] [PubMed] [Google Scholar]
- Internal laryngocele: Unusual onset in a 91-year-old female patient. Sultan Qaboos Univ Med J. 2018;18:e104-6.
- [CrossRef] [PubMed] [Google Scholar]
- Laryngopyocele presenting with acute airway obstruction. BMJ Case Rep. 2014;2014
- [CrossRef] [PubMed] [Google Scholar]
- Lateral thyrotomy approach on the paraglottic space for laryngocele resection. Laryngoscope. 2000;110:447-50.
- [CrossRef] [PubMed] [Google Scholar]
- Current diagnosis and treatment of laryngocele in adults. Otolaryngol Head Neck Surg. 2007;136:211-5.
- [CrossRef] [PubMed] [Google Scholar]




