
Translate this page into:
Awareness and prevention of anemia among pregnant women attending antenatal clinic at a University Teaching Hospital in Nigeria

*Corresponding author: Iyabo Yewande Ademuyiwa, Department of Nursing Science, Faculty of Clinical Sciences, College of Medicine, University of Lagos, Idi-Araba, Lagos, Nigeria. debbyademuyiwa@yahoo.co.uk
-
Received: ,
Accepted: ,
How to cite this article: Ademuyiwa IY, Ayamolowo SJ, Oginni MO, Akinbode MO. Awareness and Prevention of Anemia among Pregnant Women attending Antenatal Clinic at a University Teaching Hospital in Nigeria. Calabar J Health Sci 2020;4(1):20-6.
Abstract
Objectives:
During pregnancy, the fetus requires iron for blood formation so does the mother, this increases the iron requirement which is higher than that of non-pregnant women. This study assessed the level of awareness and prevention of anemia among pregnant women attending the antenatal clinic at Lagos University Teaching Hospital (LUTH), Lagos, Nigeria.
Material and Methods:
A descriptive cross-sectional study was conducted among 182 pregnant women attending the antenatal clinic at LUTH in Lagos, Nigeria. A balloting system was done to select the respondents in the clinic that runs 4 times a week, with an estimated number of 70 pregnant women per clinic. Data were collected using a structured self-administered questionnaire and analyzed with the Statistical Package of the Social Sciences version 22. Descriptive and inferential statistics were used for analysis, Chi-square test was done for the association between the variables at P < 0.05 level of significance. Ethical approval was obtained from the Human Research Ethical Committee of LUTH with approval number (ADM/DCST/HREC/APP/2589). Informed consent was taken and respondents were reassured of the privacy and confidentiality of the information obtained.
Results:
The highest percentage (33.3%) of the respondents was within the range of 26–30 years with a mean age of 28.18 ± 0.84 years. Majority of the women had a good level of awareness of anemia (68.89%) and good overall practices (73.89%) of prevention of anemia in pregnancy. There was no significant relationship between the respondents’ level of awareness of anemia and its prevention (χ2 = 1.533, P = 0.216).
Conclusion:
The study has shown that even though awareness and prevention practices were good, there is a need to create more awareness among pregnant women and also to give adequate health education on prevention of anemia to produce favorable outcome in pregnancy for both the child and mother.
Keywords
Awareness
Prevention of malaria
Pregnancy
Pregnant women
Antenatal care

INTRODUCTION
Anemia is a global public health problem affecting both low-income and lower- and middle- income countries. The World Health Organization estimated that anemia is present in 1.62 billion people worldwide, which corresponds to a prevalence of 24.8% of the population (95% CL: 22.9–26.7%),[1] and anemia in pregnancy was estimated to be 51%.[2] Sub-Saharan Africa is the most affected region with an estimated prevalence of 57% pregnant women, which corresponds to about 17.2 million affected women with severe consequences for human health as well as social and economic development. Globally, the most common cause of anemia is iron deficiency, which is responsible for about half of anemia cases in pregnancy, and it is also estimated that in developed countries 38% of pregnant women have iron depletion.[3]
Anemia occurs at all stages of the lifecycle but is more prevalent among pregnant women due to their physiological state of health.[4] Anemia in pregnancy is defined as a condition where there is less than 11g/dl of hemoglobin (Hb) concentration in the blood of pregnant woman, which decreases the oxygen-carrying capacity of the blood to the body tissues.[1] The importance of adequate Hb concentration during pregnancy for both the woman and the growing fetus cannot be overemphasized. Being a driving force for tissue oxygenation, a reduction below acceptable levels can be detrimental to both the fetus and the mother.[5]
Anemia is one of the most common nutritional deficiency disorders affecting pregnant women in developing countries. The major causes of anemia in pregnancy in developing countries are nutritional deficiencies, parasitic infestations, HIV infection, hemorrhage, and some chronic medical disorders such as renal and hepatic diseases.[6] Furthermore, infectious diseases have been reported to cause a high prevalence of anemia in sub-Saharan Africa.[7] During pregnancy, the fetus requires iron for blood formation so does the mother, this increases the iron requirements which is higher than that of non-pregnant women. Although, due to the absence of menstruation, iron requirement is reduced but begins to rise steadily thereafter from approximately 0.8 mg/day in the 1st month to approximately 10 mg/day during the last 6 weeks of pregnancy.[8]
Anemia in pregnancy usually increases the demand for iron used in blood formation. When the body is unable to meet these demands, due to either malnutrition or infection such as malaria, anemia will occur.[9] Despite increased iron requirements, pregnancy is also a period of increased risk for anemia. So far, reduction and control of anemia prevalence among women remain prioritized as public health interventions, especially in women of child-bearing age worldwide.[10] The figure of moderate and mild forms of anemia in pregnancy at booking in the antenatal clinics in Nigeria is not declining.[11]
A cross-sectional study conducted by Balasubranian et al.,[12] in Obstetrics and Gynecology Department at Government Theni Medical College and Hospital, Theni, Tamil Nadu, India. It is carried out on 600 pregnant women who were randomly selected in the antenatal clinic over a period of 6-month from June 2015 to December 2015. Women attending the antenatal clinic were obtained a verbal consent and requested to fill up the questionnaire, and 1 ml of blood was collected to assess their Hb level. The majority of the subjects were multigravida 76% and primip accounts to 24%. In the study, the literacy rate was 68%, and the illiteracy rate was 32%. The majority of the women (72%) were in the mean age of 20–29 years, teenage pregnancies (<20 years) were 18%, and elderly (>30 years) were 10%. The majority of the patients registered were in the 1st trimester. Hb level less than 11 g is taken as anemia. Out of 600 women, 459 (76.5%) are aware of anemia and 47% knows anemia is more common in pregnant women. About 53.5% of the women know about its complications and role of iron therapy (75.5%) socio- demographic factors, such as literacy rate, socioeconomic status, and iron consumption, are highly significant factors, which affect the Hb status of the study group.
A baseline survey was conducted by Dwumfour-Asare and Kwapong[13] on 28 pregnant women randomly selected from the first 100 consistent antenatal attendees from August to October 2011 at Brosankro Health Centre, Ghana. The results show high anemia consciousness with few respondents claiming no knowledge of the causes (3%) and effects (14%). The easily known cause of anemia is poor diet (63%), followed by malaria (26%), worms (5%), and others (6%). Meanwhile, food sources that can fight anemia are poorly known (18%). Cultural and religious beliefs in food restrictions exist and fairly a significant number of women (38%) are denied potential dietary nutrients. A study conducted on the knowledge and practice regarding prevention of anemia among pregnant mothers attending ANC in Governmental hospitals at west Shoa zone, Ethiopia.[14] Results showed that 286 pregnant women were participated in the study. Among them, only 57.3% and 50% were found to have good knowledge and poor practice, respectively, regarding the prevention of anemia during pregnancy. Crude and adjusted odds ratio done revealed that educational status, living in urban, having a nuclear family type, previous history of anemia, and good practice were significantly associated with knowledge, while educational status and having good knowledge also found to be significantly associated with the prevention of anemia.
The study conducted by Yesufu et al.[15] to determine the knowledge, attitude, and practices of the prevention of anemia in pregnancy amongst 220 pregnant women attending Antenatal Clinic at Ifako-Ijaiye General Hospital in Lagos, found that a majority (95%) of the respondents were aware of anemia in pregnancy but the mean knowledge score was 56.5%. Less than half (46.3%) of the respondents, thought that contraceptives could help prevent anemia in pregnancy by reducing closely spaced pregnancies. Only 31.8% were compliant with the use of iron supplements. About one third (33.2%) did not combine drinking tea with meals, while 47.3% of the respondents did not use iron supplements with milk products. The study showed that most of the respondents had a moderate level of knowledge, and positive attitude toward contraceptive use but a high proportion were not compliant with the daily use of iron supplements.
A retrospective study was conducted among pregnant women accessing antenatal care in a mission hospital in South-South Nigeria; the authors reported a prevalence of 32.3% for anemia in pregnancy at booking.[16] Researchers found the prevalence of anemia in pregnancy, at booking, to be 40.4% in Enugu, Southeastern Nigeria. Anemia was of the mild form in 90.7% of these women while moderate anemia accounted for 9.3% of cases. In a study of the socio-demographic determinants of anemia in pregnancy in Oyo State Southwestern Nigeria, researchers reported a prevalence of 32.8% for anemia in pregnancy.[17] A cross- sectional study reported a prevalence of 35.3% for anemia in pregnancy at booking in a tertiary center in Lagos, Southwest Nigeria.[11] A study conducted by Adznam et al.[18] to determine knowledge, attitude, and practice levels regarding anemia among pregnant women in Putrajaya. The result of the study showed that knowledge had no significant relationship with practice. Anemia during pregnancy is commonly associated with poor pregnancy outcome and can result in complications that threaten the life of both mother and fetus.[19] Despite the national health policy of routine iron supplementation and intermittent preventive treatment for malaria with anti-malarial drugs, still maternal anemia continues to be a common cause of morbidity and mortality. Therefore, this study assessed the awareness and prevention of anemia among pregnant women attending the antenatal clinic of an urban teaching hospital in southwest Nigeria.
MATERIALS AND METHODS
The study adopted a descriptive cross-sectional research design. Data were collected with a self-administered questionnaire that was developed through an intensive literature search. The study was carried out in Lagos University Teaching Hospital (LUTH), Idi-Araba, Lagos, Nigeria. LUTH was founded and established in the year 1912 in the outskirts of Surulere, Lagos in Mushin Local Government Area. The hospital has a total of 761 beds and 28 wards. The hospital trains hundreds of nursing, medical, dental, pharmacy, physiotherapy, radiography, and other science students. The hospital has about 13 clinical departments, on145 consultants, 400 resident doctors, and about 250 house officers giving a total of 695 doctors and 600 nurses with an average of 16 nurses on each ward. The study population included pregnant women attending the ANC in the above hospital. The antenatal unit of the hospital has four clinics days in a week with about 70 women attending in a week. The estimated number of pregnant women in a month is about 280, according to LUTH, ANC register (2020).
The minimum sample size was determined using[20] formula with a calculated sample size of 182 women after addition of a 10% non-response rate as follows:
Where;
N=Population size=280
e=Level of precision expected data 95% confidence level = 0.05
n=Required sample size.
n=165
In addition 10% attrition rate; 10% of 165 = 16.5
Total = 165+16.5= 181.5 approximately 182.
Simple random sampling technique was used to select the pregnant women that participated in the study. A balloting system with papers containing “YES” or “NO” was used to pick the participating pregnant women and to give every pregnant woman an equal chance of being selected for the study until desired sample size was achieved. A structured self- administered questionnaire was used for data collection. A pre-test was carried out on 18 pregnant women at the antenatal clinic in Lagos State University Teaching Hospital, with the Cronbach’s alpha result of reliability index of 0.78. Measurement error was eliminated to ensure the reliability of the instrument. A total number of 182 questionnaires were distributed to pregnant women, 180 questionnaires were adequately filled and returned giving a response rate of 98.8%.
Data analysis was performed with the Statistical Package of the Social Sciences (SPSS version 22.0). Fifteen items were scored for women awareness of anemia in pregnancy. The maximum obtainable score was 15 and a score of one was awarded to every correct answer while a score of zero was awarded to every wrong answer. Respondents that scored within 9–15 were categorized as good awareness and scores between 0 and 8 as poor awareness. Seven items were scored for the prevention of anemia in pregnancy with a maximum obtainable score of 35. The score was awarded as never = 1, rarely = 2, sometimes = 3, often = 4, always = 5, and vice versa for wrong answers. Respondents that scored within 20– 35 were categorized as good overall practice and those that scored within 1–19 as poor overall practice of prevention of anemia in pregnancy. Descriptive and inferential statistics were used to present the data. Chi-square test was used to compare the association between the categorical variables at P < 0.05 for statistical significance. Ethical approval was obtained from the Ethical committee of LUTH with an approval number ADM/DCST/HREC/APP/2589. Informed consent was taken from the respondents after appropriate explanation of the purpose of the study and respondents were reassured of the confidentiality of the information obtained.
RESULTS
Findings on demographic variables revealed that 60 (33.3%) of the respondents were within the range of 26–30 years of age and the mean age was 28.16 ± 0.84 years. About 77 (42.8%) were Yoruba, and majority 151 (83.9%) of the respondents were married. Furthermore, 97 (53.9%) of the respondents were government or private employed, 33 (18.3%) earned an income of less than 10,000 monthly, few respondents 43 (23.9%) earned >50,000 naira monthly. More than half of the respondents 96 (53.3%) had finished a tertiary level of education, as shown in Table 1.
| Variables | Frequency (n=180) | Percentage |
|---|---|---|
| Age (mean age=28.16±0.84) <21 | 10 | 5.6 |
| 21–25 | 52 | 28.9 |
| 26–30 | 60 | 33.3 |
| 31–35 | 45 | 25.0 |
| 36–40 | 11 | 6.1 |
| >40 | 2 | 1.1 |
| Total | 180 | 100.0 |
| Ethnic group | 60 | 33.3 |
| Igbo | 77 | 42.8 |
| Yoruba | 31 | 17.2 |
| Hausa | 12 | 6.7 |
| Others | 180 | 100.0 |
| Total | ||
| Marital status | 33.3 | 83.9 |
| Married | 42.8 | 12.8 |
| Single Widowed | 17.2 6.7 | 1.1 2.2 |
| Divorced | 100.0 | 100.0 |
| Total | ||
| Occupation | 68 | 37.8 |
| Self-employed (business) | 97 | 53.9 |
| Government or private employed | 15 | 8.3 |
| Others | 180 | 100.0 |
| Total | ||
| Income (Naira) | ||
| <10,000 | 151 23 | 18.3 25.0 |
| 10,000–30,000 | 2 | 32.8 |
| 30,000–50,000 | 4 | 23.9 |
| >50,000 | 180 | 100.0 |
| Total | ||
| Educational level | 23 | 12.8 |
| Primary | 61 | 33.9 |
| Secondary | 96 | 53.3 |
| Tertiary | ||
| Total | 180 | 100.0 |
Table 2 shows that 140 (77.8%) respondents have heard of anemia, 76 (42.2%) of them could correctly define anemia, and 129 (71.7) of them could correctly identify different causes of anemia. Many 80 (44.4%) respondents correctly identified the signs and symptoms of anemia as (the skin appear pallor and paleness of the conjunctiva, palm, tongue, general body malaise, heart palpitation, and fatigue). A majority 135 (75%) of the respondents identified that anemia can be treated and 117 (65%) identified the right means of treatment using hospital treatment. Seventy- nine (43.9%) respondents identified the correct means of preventing anemia (eating meat, eggs, green vegetables, and fruit). A majority 137 (94.5%) of the respondents agreed that anemia can cause a serious problem for them and their expected baby. One hundred and thirty-one (72.8%) of the respondents identified correctly, the complications of anemia for both mother and fetus. A majority 115 (63.9%) of the respondents identified reduced iron dietary intake as a cause of anemia. A majority 141 (78.3%) of the respondents put what they have learnt in the antenatal clinic to practice.
| Items | Frequency (n=180) | Percentage |
|---|---|---|
| Have you heard of anemia in pregnancy | 140 | 77.8 |
| What anemia means is a decrease in the concentration of red blood cell or hemoglobin level in the blood | 76 | 42.2 |
| How can one get anemia (poor dietary intake, parasitic infections, and chronic infections, i.e., T.B and HIV, reproductive cause, and genetic blood disorders) | 129 | 71.7 |
| How can one know that she is suffering from anemia (the skin appear pallor and paleness of the conjunctiva, palm, tongue, general body malaise, heart palpitation, and fatigue) | 80 | 44.4 |
| Can anemia be treated (yes) | 135 | 75 |
| If yes, how is anemia treated (using hospital treatment) | 117 | 65 |
| How can one protect herself from getting anemia (eating meat, eggs, green vegetables, and fruit) | 79 | 43.9 |
| Can anemia cause a serious problem in your health and for expected baby (yes) | 137 | 94.5 |
| What are the complications of anemia for both mothers and fetus (low birth weight, preterm delivery, still-birth, and death may occur) | 131 | 72.8 |
| Which of the following can cause anemia during pregnancy (reduced iron dietary intake) | 115 | 63.9 |
| In antenatal clinic, the health-care provider usually provides health education on anemia in pregnancy | 141 | 78.3 |
Figure 1 shows that 31.1% of the respondents had poor awareness of anemia while 68.9% had a good awareness of anemia, which indicates that a majority of the respondents had a good awareness of anemia.

- Pie chart showing the overall awareness of anemia.
Table 3 shows that the majority of the respondents sometimes boil their water before drinking 40.6%. The majority of the respondents also sometimes eat a diet rich in iron such as liver, snail, and vegetables. Furthermore, the majority of the pregnant women visit the antenatal clinic often visits the antenatal clinic 43.3% and most of them sometimes put into practice what was taught at the antenatal clinic.
| Variables | Never (%) | Rarely (%) | Sometimes (%) | Often (%) | Always (%) |
|---|---|---|---|---|---|
| Frequency of intake of balanced meal | 0 (0) | 2 (1.1) | 85 (47.2) | 53 (29.4) | 40 (22.2) |
| Frequency of taken foods rich in dietary iron, for example, liver, snail, orange, and vegetables | 0 (0) | 2 (1.1) | 96 (53.3) | 50 (27.8) | 32 (17.8) |
| Use of insecticide treated net | 4 (2.2) | 50 (27.8) | 51 (28.3) | 24 (13.3) | 51 (28.3) |
| Boiling of water before you drink | 8 (4.4) | 59 (32.8) | 73 (40.6) | 21 (11.7) | 19 (10.6) |
| Visiting the antenatal clinic | 4 (2.2) | 6 (3.3) | 47 (26.1) | 78 (43.3) | 45 (25) |
| Putting what you have learnt at the clinic into practice | 7 (3.9) | 6 (3.3) | 87 (48.3) | 38 (21.2) | 42 (23.3) |
| Culture and belief affect your prevention of anemia | 78 (43.3) | 59 (32.8) | 33 (18.3) | 0 | 10(5.6) |
Figure 2 shows that 73.9% of the respondents have good overall practices of prevention of anemia while 26.1% have poor overall practices of prevention of anemia. A total score of 35 was allocated to each. Those that scored less than 20 had poor overall practice of prevention of anemia while those who had 20 and above had a good overall practice of prevention of anemia.
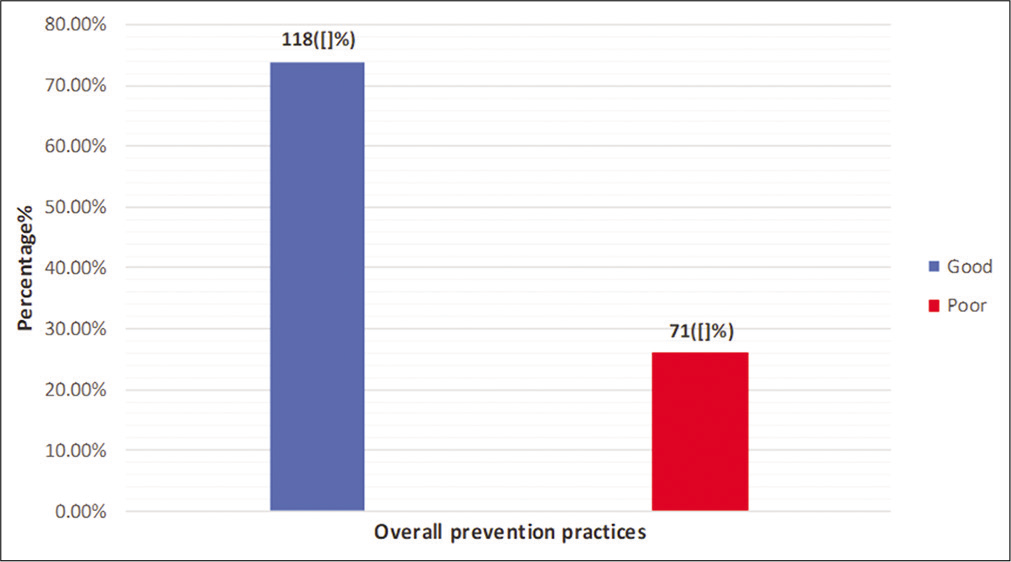
- Overall anemia prevention practices.
Table 4 revealed no significant relationship between the respondents’ awareness of anemia and its prevention practices (χ2 =1.533, P = 0.216).
| Prevention practices | Awareness of anemia in pregnancy | Total (%) | χ2 | df | P-value | |
|---|---|---|---|---|---|---|
| Poor (%) | Good (%) | |||||
| Poor | 11 (23.4) | 36 (76.6) | 47 (100) | 1.533 | 1 | 0.216 |
| Good | 44 (33.1) | 89 (66.9) | 133 (100) | |||
| Total | 55 (30.6) | 125 (69.4) | 180 (100) | |||
DISCUSSION
The findings of the study show that the respondents were within the age range of 26–30 years of age with a mean age of 28.18 ± 0.84 years which is in agreement the report of the study conducted by Duko et al.,[21] where the majority of the respondents were within the age range 26-30 years. It is not surprising that the majority of respondents were Igbos because the study area is inhabited predominantly by people of the Igbo ethnic group. The Igbos who is the second largest ethnic group is known to be renowned traders who often constitute a significant portion of the populations in most major cities in Nigeria. The vast majority of the respondents were married. However, few pregnant women were single. Hence, this reflected the much respected value of the institution of marriage in Lagos State. Most (50%) of the respondents had tertiary education and this finding may also be due to where the study was conducted being a tertiary health institution where more educated people will prefer to register because of access to more specialized care in the case of any emergency or complication in pregnancy or at childbirth.[22]
The findings of this study show that majority of the respondents reported a good awareness of anemia. This finding contrasts with the report of Duko et al.[21] where only 44.3% (102) of respondents had comprehensive awareness of anemia. A descriptive study carried out on knowledge, attitude, and practices regarding the prevention of iron deficiency anemia (IDA) among pregnant women also reported poor knowledge of IDA among the majority of respondents.[23] The study on knowledge, attitude, and practices of prevention of anemia in pregnancy amongst pregnant women attending the Antenatal Clinic at Ifako- Ijaiye General Hospital, Lagos, Nigeria conform to the present study in their finding of majority (95%) of respondents being aware of anemia in pregnancy.[15]
The findings of this study reveal that a majority of the respondents had a good overall practice of prevention of anemia (which includes boiling drinking water, eating a balanced diet, eating a diet rich in iron, and sleeping under insecticide-treated nets). This finding is in accordance with a study conducted by Keneni et al.,[14] to assess the knowledge and practices regarding the prevention of anemia among pregnant mothers attending ANC in Governmental hospitals at west Shoa zone, in Ethiopia, where 286 pregnant women participated in the study, the authors found that 50% of the respondents had poor practice regarding prevention of anemia during pregnancy. Similarly, the result of this study is in agreement with a descriptive study carried out to evaluate knowledge, attitude, and practice regarding prevention of IDA among pregnant women attending primary health centers in Tabuk region.[23] The findings revealed that 40.0% of them had poor practice score regarding the prevention of IDA. The result of this study also differs with a cross-sectional descriptive study carried out to assess the knowledge, attitude, and practice of pregnant mother toward the prevention of IDA in Ethiopia. Total of 128 mothers was interviewed with a mean age of 26.3 years and the majority (58.6%) having poor adherence to prevention practice of IDA.[24]
Moreover, the findings from this study show that there was no significant relationship between awareness of anemia and its prevention among pregnant women in the study setting. This finding is similar to the report of Adznam et al.[18] on knowledge, attitude, and practice levels regarding anemia among pregnant women in Putrajaya, in which respondent’s knowledge had no significant relationship with the practice of prevention of malaria during pregnancy.
CONCLUSION
The study concluded that although awareness and prevention practices of anemia in pregnancy were good. There is a need to create more awareness on anemia in pregnancy and effective health education programs on the prevention of anemia to achieve a more favorable fetomaternal outcome in pregnancy.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Global Nutrition Targets 2025, Anaemia Policy Brief, Targets 50% Reduction of Anaemia in Women of Reproductive Age Geneva: World Health Organization; 2014.
- [Google Scholar]
- Prevalence and predictors of maternal anemia during pregnancy in Gondar, Northwest Ethiopia: An institutional based cross-sectional study. Anemia. 2014;2014:108593.
- [CrossRef] [PubMed] [Google Scholar]
- Nutrition Technical Brief: A Simple Method for Making a Rapid, Initial Assessment of the Consumption and Distribution of Iron-Folic Acid Supplements among Pregnant Women in Developing Countries. USAID/ Strengthening Partnerships, Results and Innovations in Nutrition Globally (SPRING) Project.
- [Google Scholar]
- Prevalence and associated factors of anemia among pregnant women of Mekelle Town: A cross sectional study. BMC Res Notes. 2014;7:888.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence of anaemia among pregnant women at booking in the University of Uyo teaching hospital, Uyo, Nigeria. Biomed Res Int. 2014;2014:849080.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence and risk factors of anaemia among pregnant women in Nigeria. Open Haematol J. 2012;2:14-9.
- [CrossRef] [Google Scholar]
- Prevalence of anemia and associated risk factors among pregnant women attending antenatal care in Azezo Health Center Gondar town, Northwest Ethiopia. J Interdiscipl Histopathol. 2013;1:137-44.
- [CrossRef] [Google Scholar]
- Malaria and anaemia in pregnant and non-pregnant women of child-bearing age at the University Hospital, Kumasi, Ghana. Open J Med Microbiol. 2013;3:193-200.
- [CrossRef] [Google Scholar]
- Maternal knowledge, food restriction and prevention strategies related to anaemia in pregnancy: A cross-sectional study. Int J Community Med Public Health. 2015;2015:331-8.
- [CrossRef] [Google Scholar]
- Anaemia in pregnancy and challenges. J South Asian Fed Obstet Gynaecol. 2012;1:64-70.
- [CrossRef] [Google Scholar]
- Anemia in pregnancy and its associated factors among primary care clients in Sagamu, Southwest, Nigeria: A facility-based study. J Family Med Prim Care. 2017;6:323-9.
- [CrossRef] [PubMed] [Google Scholar]
- Awareness of anaemia among pregnant women and impact of demographic factors on their haemoglobin status. Int Sci Stud. 2016;3:303-5.
- [Google Scholar]
- Anaemia awareness, belief and practices among pregnant women: A baseline assessment at brosankro community in Ghana. J Nat Sci Res. 2013;3:2224-3186.
- [Google Scholar]
- Assessment of knowledge and practice towards prevention of anemia among pregnant women attending antenatal care at government hospitals in West Shoa Zone, Ethiopia. J Health Med Nurs. 2018;50:31-40.
- [Google Scholar]
- Anaemia prevention in pregnancy among antenatal clinic attendees in a general hospital in Lagos. Nig Q J Hosp Med. 2013;23:280-6.
- [Google Scholar]
- Effects of nutritional educational guideline among pregnant women with iron deficiency anaemia at rural areas in Kalyobia Governorate. Life Sci J. 2012;9:1212-7.
- [Google Scholar]
- Haematocrit, anemia, and arm preference for blood sample collection: A cross-sectional study of pregnant women in Enugu, South-Eastern, Nigeria. Ann Med Health Sci Res. 2015;5:36-40.
- [CrossRef] [PubMed] [Google Scholar]
- Assessment of Knowledge, attitude and practice levels regarding anaemia among pregnant women in Putrajaya, Malaysia. Pak J Nutr. 2018;17:578-85.
- [CrossRef] [Google Scholar]
- Prospective study on prevalence of anaemia of pregnant women and its outcome. J Family Med Prim care. 2017;6:739-43.
- [CrossRef] [PubMed] [Google Scholar]
- Awareness of anemia and associated factors among pregnant women attending antenatal care, South Ethiopia. J Womens Health Care. 2017;6:1000409.
- [Google Scholar]
- Birthing Centers and Hospital Maternity, Kids Health United States: Nemours Foundation; 2019.
- [Google Scholar]
- Knowledge, attitude and practice regarding prevention of iron deficiency anemia among pregnant women in Tabuk region. Int J Pharm Res Allied Sci. 2019;8:87-97.
- [Google Scholar]
- Knowledge, attitude and practice of pregnant mothers towards preventions of iron deficiency anemia in Ethiopia: Institutional based cross sectional study. Health Care. 2019;7:1-7.
- [CrossRef] [Google Scholar]




