
Translate this page into:
Treatment outcome of appendicitis in Azare
 , Sani Adamu3, Aminu Muhammed Umar1, Jatto Kabir Busayo2, Oaikhena John Okoruwa1
, Sani Adamu3, Aminu Muhammed Umar1, Jatto Kabir Busayo2, Oaikhena John Okoruwa1

*Corresponding author: Kefas John Bwala, Department of Surgery, Abubakar Tafawa Balewa University Teaching Hospital, Bauchi, Nigeria. kefbwala@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Bwala KJ, Giade AS, Yusuf S, Adamu S, Umar AM, Busayo JK, et al. Treatment outcome of appendicitis in Azare. Calabar J Health Sci 2023;7:25-8.
Abstract
Objectives:
Appendicitis is and has remained one of the most common abdominal surgical emergencies the world over. Its procedure and appendectomy is also a very common and regularly done surgical procedure and, thus, a very important disease to describe in totality. Hence, we set out to describe the pattern of presentation and management outcome of this condition in our environment.
Materials and Methods:
Data were collected retrospectively of all patients with the clinical diagnosis of appendicitis during the study period and analyzed.
Results:
A total of 62 patients had a clinical diagnosis of appendicitis over the period under review. M: F was 1:1.1. Age ranged from 3 years to 47 years with a mean of 21.50 ± 10.07. All (100%) patients presented with right iliac fossa pain. Other symptoms were anorexia (45.2%), nausea (61.3%), and vomiting (40.3%). All (100%) of patients went on to have an appendectomy. Twelve (19.40%) patients had surgical site infection and 2 (3.20%) developed enterocutaneous fistula. Duration of hospital stay ranged from 1 to 30 days. One patient who had uncontrolled diabetes mellitus died giving a mortality rate of 1.6.
Conclusion:
Typical clinical features of acute appendicitis were lower abdominal quadrant pain associated with nausea, anorexia, and vomiting. It goes without saying that diagnosis can still be made comfortably on clinical grounds and treatment outcome is generally good.
Keywords
Appendicitis
Pattern
Treatment outcome

INTRODUCTION
Typhlitis refers to acute inflammation of the caecum/vermiform appendix and was first recognized by Fitz in 1886.[1] It is now widely known as acute appendicitis and remains the most common cause of acute surgical abdominal conditions worldwide.[2-4] Clinical diagnosis can be made with great accuracy, although various scoring systems such as the Alvarado scoring system have been devised to reduce the incidence of negative appendicectomy.[5,6]
In developed countries where advanced cross-sectional imaging is readily available, it has a specificity of 93–99% and sensitivity of 95–97%, but the risk of exposure to radiation is a drawback, especially in children. Ultrasound scans can be used but with less accuracy and highly subjective and observer-dependent. Thus, in our setting here, (and many other developing and resource-poor regions of the world), we still rely mostly on clinical presentations to make diagnosis.
The treatment of acute appendicitis is appendectomy and it can be an open or laparoscopic procedure.
The aim of this study is to describe the pattern of presentation and management outcome of acute appendicitis in our environment.
MATERIAL AND METHODS
Federal Medical Center (FMC) Azare is a tertiary hospital located in Azare town of Bauchi state North East Nigeria. Ethical approval was obtained from the Research and Ethics Committee of the Hospital. This was a retrospective study of all patients with the clinical diagnosis of acute appendicitis seen at FMC Azare over 2 years (January 1, 2012–December 31, 2013). Relevant data which included age, sex, symptoms and signs, intraoperative findings, postoperative complications, and outcome of surgery were extracted from their folders and entered into a structured pro forma. The information was coded and entered into statistical package for social sciences (SPSS) version 25 which was used to analyze the data. Means and standard deviations were used to analyze quantitative variables, as well as graphs and charts. The chi-square test was used for inference and a value <0.05 was considered significant.
RESULTS
Within the 2 years, a total of 62 patients presented and had a diagnosis of acute appendicitis in the facility. There were 30 males and 32 females making the male-to-female ratio 1:1.1. The youngest patient was 3 years and the oldest was 47 years with a median age of 21.5 and a peak age incidence was in the third decade (20–29). Age and sex distribution is shown in [Table 1].
| Age (years) | Sex | Total (%) | |
|---|---|---|---|
| M | F | ||
| 0–9 | 1 | 2 | 3 (4.8) |
| 10–19 | 10 | 12 | 22 (35.5) |
| 20–29 | 8 | 15 | 23 (37’1) |
| 30–39 | 5 | 2 | 7 (11.3) |
| 40–49 | 6 | 1 | 7 (11.3) |
| Total (%) | 30 | 32 | 62 (100) |
The duration of symptoms before presentation ranged from 1 to 14 days with the most common symptom being right-sided lower abdominal pain in which the initial site before it settles in the right abdomen can be seen in Figure 3. Other symptoms are nausea 38 (61.30%) and anorexia 28 (45.20%). Only 7 (11.3%) patients presented within 24 h of the onset of symptoms. The most common sign elicited was right lower abdominal quadrant tenderness 53 (85.5%) with rebound tenderness and guarding occurring in an equal proportion of 34 (54.8%). Other signs and symptoms are shown in [Figures 1 and 2]. The diagnosis of acute appendicitis was made clinically on the history of periumbilical pain or discomfort with a shift to the right lower abdominal quadrant associated with or without rebound tenderness. Fifty-three (85.5%) patients had right iliac fossa (RIF) tenderness followed by rebound tenderness and guarding 34 (54.80%) each. The average leucocyte count for those with ruptured appendix was 15.2 × 109/L and for those with inflamed appendix was 13.8 × 109/L.

- Signs of patient at presentation.

- Symptoms of patient at presentation.
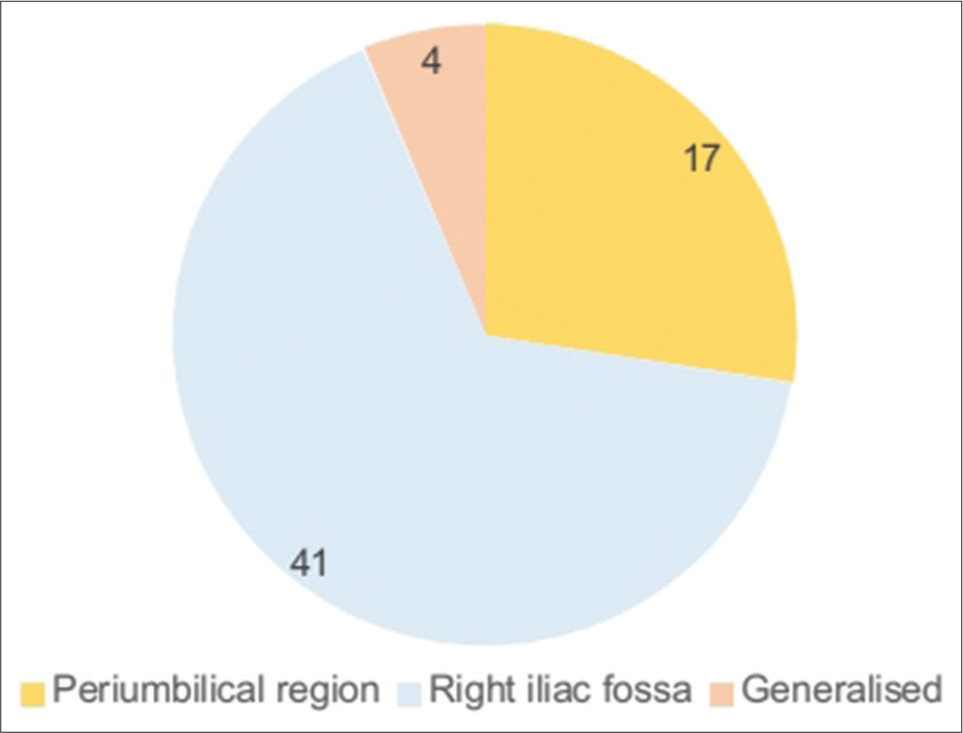
- Site of initial abdominal pain at presentation.
All 62 (100%) patients went on to have an open appendectomy, with the Lanz incision being the most common type of incision used in 21 (33.90%) patients due to its cosmetically acceptable outcome. Other types of incisions used are shown [Table 2]. Intraoperative finding of inflamed appendix was seen in 36 (58.10) patients, while 13 (21.00%) had ruptured appendix. One patient stayed on admission for 30 days before discharge after he developed an enterocutaneous fistula and was managed non-operatively. One patient who is a 27-year known type 1 diabetic mellitus patient with poorly controlled sugar level died giving a mortality rate of 1.6.
| Type of incision | Frequency | Percentage |
|---|---|---|
| Grid iron | 18 | 29.0 |
| Lanz | 21 | 33.9 |
| Paramedian | 3 | 4.8 |
| Lower midline | 20 | 32.3 |
| Total | 62 | 100.0 |
DISCUSSION
Appendicitis is the most common acute surgical abdominal condition worldwide with an estimated incidence of 5.7– 50/100,000.[7] Some researchers have reported higher male preponderance,[8,9] which is at variance with our findings that demonstrated slight female preponderance over males, M: F ratio of 1:1.1. This is however in keeping with most other studies.[10,11] The peak age incidence is in the third decade (20–29 years) as reported in multiple other studies including Ali et al.[11] Similarly, 90% of our patients were 40 years and below. An alternative hygiene hypothesis by Baker may be responsible for the increased incidence of acute appendicitis at age 40 and below.[12]
The clinical features as seen in [Figures 1 and 2] are similar to most previous studies. Right lower quadrant abdominal pain was seen in all our patients, other symptoms were anorexia, nausea, and vomiting. Bowel habit changes such as diarrhea and constipation was found in 4.8% and 11.3%, respectively. This is in agreement with reports by other authors including Deneke et al. who reported diarrhea and constipation in 7.6% and 6.9% of their patients, respectively.[13] RIF tenderness was seen in only 85.5% and this is at variance with the findings of a study in Ibadan where all their patients had RIF tenderness.[14] Rebound tenderness was seen in 54.8% similar to the one in Ibadan.[14] Fever was seen only in 35.5%, most patients with uncomplicated appendicitis hardly present with fever.
The duration of symptoms before hospital presentation ranged from 1 to 14 days. The delay in presentation is related to a high incidence of complicated appendicitis. This underscores the importance of early presentation and surgical intervention. It has been observed that the duration of symptoms was not related to age or gender but rather related to the incidence of complicated appendicitis which may indicate that most of the perforations occurred before hospital admissions.[15] We used a slightly modified Alvarado score [Table 3] in categorizing the patients by excluding one laboratory parameter: Shift to the left of neutrophils maturation (score 1) similar to the study by Kalan et al.[16] This was not available from our laboratory on a routine basis, and therefore, our patients were scored out of 9 rather than 10 points. Patients with scores of 7–9 underwent an appendicectomy, while those with a score of <7 were not considered for surgery. Alvarado scoring system as seen in [Table 3] was devised to reduce the chances of negative appendectomies. Surgical site infection defined as discharge of pus from the wound site was the most common complication occurring in 18.4% of cases mostly in those that had ruptured appendicitis as seen in [Figure 4], similar to what Ohene-Yeboah and Togbe[17] reported but different from the reports by Ali and Aliyu in Maiduguri.[11] The overall complication rate was 24.2% similar to other findings.[9,17]
| Variable | Value |
|---|---|
| Symptoms | |
| Migration of pain | 1 |
| Anorexia | 1 |
| Nausea/vomiting | 1 |
| Examination | |
| Right lower quadrant tenderness | 2 |
| Rebound pain | 1 |
| Elevation of temperature ≥37.3°C | 1 |
| Laboratory | |
| Leukocytosis ≥10×10^9/L | 2 |
| Total 9 |

- Post-operative complications.
While the mortality rate in most series has reduced to <1%, ours is 1.6%, this may not be unconnected with the delay in seeking medical attention. Morbidity still remains high especially wound infection which may be due to delay in presentation leading to complications. Early presentation with the early surgical intervention before perforation occurs may reduce this high rate of post-operative complications.
CONCLUSION
The presentation of acute appendicitis in FMC Azare (in Bauchi state, the northeastern part of Nigeria) is similar to the ones earlier reported in other parts of Africa with the peak age incidence in the third decade. Clinical presentation and examination features remain the major step necessary for accurate diagnosis and early diagnosis with prompt surgical intervention may reduce postoperative complications.
Limitations
We would have loved to add the histological pattern of the appendix, but this was not used for analysis, because for the period under review, we do not have a histopathologist so tissue samples were preserved in formalin and given to patients to take it to a nearby tertiary hospital for processing and most time patients did not come back with the results. Sometimes, they will even go and bury the tissue sample.
Acknowledgment
We acknowledge with thanks the valuable contribution of Dr. Abdullahi M. Kirfi for assisting in entering the data into SPSS.
Declaration of patient consent
The Institutional Review Board (IRB) permission was obtained for the study.
Conflicts of interest
There are no conflicts of interest.
Financial support and sponsorship
Nil.
References
- Epidemiologic features, seasonal variations and false positive rate of acute appendicitis in Shahr-e-Rey, Tehran. Int J Surg. 2007;5:95-8.
- [CrossRef] [PubMed] [Google Scholar]
- The burden of appendicitis-related hospitalizations in the United States in 1997. Surg Infect (Larchmt). 2004;5:160-5.
- [CrossRef] [PubMed] [Google Scholar]
- Clinical spectrum of acute abdominal pain in Accra, Ghana. West Afr J Med. 1999;18:13-6.
- [Google Scholar]
- Alvarado versus RIPASA score in diagnosing acute appendicitis. Rawal Med J. 2013;38:147-51.
- [Google Scholar]
- Modified Alvarado scoring system in the diagnosis of acute appendicitis. Ann Punjab Med Coll. 2008;2:91-4.
- [Google Scholar]
- Diagnosis and treatment of acute appendicitis: 2020 update of the WSES Jerusalem guidelines. World J Emerg Surg. 2020;15:27.
- [CrossRef] [PubMed] [Google Scholar]
- Pattern of presentation and outcome of management of acute appendicitis: A 10-year experience. J Clin Sci. 2018;15:171-5.
- [CrossRef] [Google Scholar]
- Appendicitis in Kano, Nigeria: A 5-year review of pattern, morbidity and mortality. Ann Afr Med. 2004;3:38-41.
- [Google Scholar]
- Appendicitis in university of Port Harcourt teaching hospital, Nigeria. East Afr Med J. 2012;89:327-31.
- [Google Scholar]
- Appendicitis and its surgical management experience at the University of Maiduguri teaching hospital Nigeria. Niger J Med. 2012;21:223-6.
- [Google Scholar]
- Acute appendicitis and dietary fibre: An alternative hypothesis. Br Med J (Clin Res Ed). 1985;290:1125-7.
- [CrossRef] [PubMed] [Google Scholar]
- Pattern and clinical presentation of acute appendicitis in adults in Zewditu Memorial Hospital. Ethiop J Health Sci. 2003;13:117-23.
- [Google Scholar]
- Incidence of acute nonperforated and perforated appendicitis: Age-specific and sex-specific analysis. World J Surg. 1997;21:313-7.
- [CrossRef] [PubMed] [Google Scholar]
- Evaluation of the modified Alvarado score in the diagnosis of acute appendicitis: A prospective study. Ann R Coll Surg Engl. 1994;76:418-9.
- [Google Scholar]
- An audit of appendicitis and appendicectomy in Kumasi, Ghana. West Afr J Med. 2006;25:138-47.
- [CrossRef] [PubMed] [Google Scholar]




