
Translate this page into:
Anatomic imaging study of luminal diameter of the circle of Willis in patients with ischemic stroke
 , Charles Chibunna Ani4, Ulu Ulu Okoro4, Nneoyi Onen Egbe1
, Charles Chibunna Ani4, Ulu Ulu Okoro4, Nneoyi Onen Egbe1
-
Received: ,
Accepted: ,
How to cite this article: Paulinus SO, Udoh BE, Efanga SA, Udo-Affah GU, Eru EM, Ani CC, et al. Anatomic imaging study of luminal diameter of the circle of Willis in patients with ischemic stroke. Calabar J Health Sci 2021;5:75-80.
Abstract
Objectives:
Stroke or cerebrovascular accident is associated with defects in the circle of Willis; the vascular network that supplies the brain. There is currently lack of literature on the involvement of the circle of Willis in patients with stroke or its association with impending stroke. The objective of the study was to evaluate luminal diameter of arteries that constitute the circle of Willis in patients with stroke using computed tomography angiography (CTA) and magnetic resonance imaging (MRI) scans.
Material and Methods:
Angiograms of 340 male and female patients aged 15–>75 (40.18 ± 1.1 and 43.68 ± 1.18) years with suspected stroke, referred for either brain CTA or MRI in selected hospitals/diagnostic centers in Nigeria were evaluated using RadiAnt and the MicroDicom viewer software applications. A retrospective descriptive research design was adopted with approval from the federal health research ethics committee. Direct measurement of luminal diameter of major arteries of the circle of Willis was done using SPSS version 25 at P < 0.05.
Results:
From the 340 images assessed, 256 (75.29%) patients had ischemic stroke with luminal diameter of arteries of the circle of Willis ranged from 1 mm to >3 mm while 84 (24.71%) patients were without stroke with luminal diameter ranged from 1 mm to 2.11 mm (P < 0.05).
Conclusion:
Patients with stroke have larger luminal diameter of arteries that form the circle of Willis when compared to patients without stroke. The study has established for the 1st time, luminal diameter of circle of Willis that may be an index in the sampled Nigerian population.
Keywords
Circle of Willis
Computed tomography angiography
Ischemic stroke
Luminal diameter
Magnetic resonance imaging

INTRODUCTION
The circle of Willis is the major arterial supply to the human brain, a complex structure first described and named after a 17th century English Physician, Doctor Thomas Willis in the year 1664.[1-4] A classical, standard, or complete pattern of the circle of Willis, where all vessels are intact, is crucial for an upkeep of persistent supply of blood to the brain.[5-7] Any changes or defects in its structure may cause vascular inefficiency, which may predispose the individual to stroke with attendant secondary consequences.[8,9] Stroke or cerebrovascular accident occurs when blood flow to the brain is disrupted, due to blood clot or rupture of cerebral vessels, cutting off the supply of oxygen and nutrients leading to damage of the brain tissues.[10,11] The effect of stroke depends on severity of the injury and the extent of damage to the brain segment affected. The prognosis also depends on severity and how fast treatment interventions are performed.[12,13] However, a very severe stroke can lead to sudden death.[11,12] Stroke may be of the ischemic and the hemorrhagic types, with the ischemic type responsible for about 87% of cases.[11] Stroke is associated with defects in the circle of Willis; the vascular network that supplies the brain.[8,12] The hemodynamics of the circle of Willis is predisposed by variants in caliber of sections that affect its major role as an anastomotic channel.[10,14] A study reported that the right segment of the circle of Willis had larger diameter than the left but another similar work observed that vascular diameter (in millimeters) according to age and gender on the left side was larger than the right.[15,16] These differences in diameters and segments may provide important information on caliber of the circle of Willis for better interpretation of angiographic images and for a deeper understanding of cerebral pathology such as stroke.[8,17] Studies have shown that arteries of circle of Willis measured with methods such as cadaveric gross dissection, injection technique, and the use of computed tomography angiography (CTA) and the magnetic resonance imaging (MRI) scans in male and female individuals recorded normal vascular dimensions. This ranged from 1 mm to 3 mm.[8,15-22] Another similar work recorded diameter of the anterior cerebral artery (ACA) on MRI angiograms. This ranged from 1 mm to 2.5 mm (1.72 ± 0.45 mm).[23] In addition, a study reported that the diameter of the right ACA ranged from 1.35 mm to 2.62 mm (2.31 mm ± 0.72 mm) whereas, on the left, the range was from 1 mm to 2.93 mm (2.08 mm ± 0.42 mm).[8] The present research observed that the aforementioned studies focused on only the ACA but did not consider luminal diameter of other major arteries which include the middle cerebral artery (MCA), the posterior cerebral artery (PCA), and the basilar artery (BA) that also form the circle of Willis. Neuroimaging, using advanced modalities such as computed tomography and MRI scans, has become very useful in identifying defects affecting the circle of Willis and the entire brain.[10,14] For example, the non-contrast computed tomography (CT) can easily be extended to CTA or MRI circle of Wills using the time-of-flight (TOF) sequence for MRI within a 5–10 min examination.[10,24] This has been effectively integrated into the acute stroke imaging protocol.[25,26] Therefore, CTA protocol and the MRI TOF sequence may proffer significant information on stroke management.[1,3] However, the role of these tools (CTA and MRI) in the prognosis of stroke is poorly understood. Thus, an understanding of the luminal diameters/dimensions of the circle of Willis associated with impending stroke, affected regions of the brain and patient outcome with the use of either CTA or MRI as diagnostic tools is crucial in designing interventions to improve patients’ outcome. Hence, the need informed the present study.
MATERIAL AND METHODS
A retrospective descriptive (cohort) study of 340 images of brain CTA and MRI of male and female referrals with suspected stroke, aged 15–>75 (40.18 ±1.1 and 43.68 ± 1.18) years, sourced from selected hospitals/ diagnostic centers with CT and MRI scanners in Nigeria [Tables 1 and 2] was employed. Approval from the Federal Health Research Ethics Committee (Approval Number: FHREC/2019/01/51/13-05-19) was obtained. A convenient non-probability sampling technique was used to select the images, assessed with installed RadiAnt Digital Imaging and Communication (DICOM), the MicroDICOM viewer software applications, and a SONY-VPCY11M1E model system type ×64-based personal computer. At the region of interest with the measurement tool for distance, the tunica intima of an axial/transverse image of the selected artery with cursor placed at a point “X” to another “Y” was used to establish the distance XY [Figure 1]. A conversion factor, according to the unit converter + software application, was used to automatically convert the pixel (×) values to millimeter (mm) for every distance measured, where 1 pixel (×) = 0.2645833333 mm. A direct measurement of luminal diameter of the major vessels of circle of Willis using archived primary images of CTA and MRI was, therefore, used as the method of data collection. The arteries evaluated were terminal branches of the internal carotid artery {ICA (ACA and MCA)}, BA, and its terminal branches, these include;

- Representation of the different points measured in circle of Willis where
- A1Rt is pre-communicating portion of the right ACA
- A1Lt is pre-communicating portion of the left ACA
- M1Rt is sphenoidal segment of the right MCA
- M1Lt is sphenoidal segment of the left MCA
- P1Rt is right segment of PCA
- P1Lt is left segment of the PCA
- BA is basilar artery
- X↔Y is the widest/largest luminal diameter measured (mm).
| Hospital/center | Name | Make | Country | Machine s/n | Date of manufacture | Output max. kVp mAs |
|
|---|---|---|---|---|---|---|---|
| A | Bright-Speed 4-Slice | GE | USA | 16507017m4 | 2007 | 140 | 300 |
| B | Optima 64 Slice | GE | USA | 369366HMO | 2014 | 140 | 800 |
| C | Brivo 385 Series 16 Slice | GE | India | 96369B14 | 2014 | 140 | 200 |
| D | Brivo 385 16-Slice | GE | China | 353806HM3 | 2013 | 140 | 180 |
CT: Computed tomography
| Hospital/center | Name | Make | Country | Date of manufacture | Output |
|---|---|---|---|---|---|
| A | Somatom | Siemens | Germany | 2007 | 0.2 Tesla |
| B | Multiva | Philips | Holland | 2016 | 1.5 Tesla |
| C | Signa Ovation | GE | USA | 2014 | 0.35 Tesla |
| D | Magnetom Concerto | Siemens | Germany | 2014 | 0.2 Tesla |
| E | Brivo 235 | GE | India | 2014 | 0.5 Tesla |
MRI: Magnetic resonance imaging
The A1 segment/pre-communicating part of the ACA (from termination of ICA to the junction with the ACoA) bilaterally
The M1/sphenoidal segment (from termination of ICA to its bi or trifurcation) bilaterally
1. The P1 segment (from basilar bifurcation to the junction with PCoA) bilaterally. During evaluation, abbreviations were used to show the different points measured [Figure 1] for easy interpretation. Data obtained were analyzed with the Statistical Package for the Social Science version 25 and the Microsoft Excel computer program. The level of significance was set at P < 0.05.
RESULTS
From the images of patients assessed, 256 (75.29%) had ischemic stroke while 84 (24.71%) cases had no stroke [Figure 2] on pattern recognition. The result [Table 3] showed that the major arteries that constitute the circle of Willis in male and female individuals without stroke had luminal diameter ranged from 1 mm to 2.11 mm [Plates 1 and 2]. This accounts for 24.71% of the total sampled images evaluated [Figure 2]. Table 3 also shows that patients (male and female) with ischemic stroke had luminal diameter of major arteries that form the circle of Willis ranged from 1 mm to >3 mm [Plate 3]. This accounts for 75.29% of the total 340 sampled images [Figure 2]. A significant difference exists between patients with stroke and individuals without stroke (P < 0.05). In addition, only the M1 segment of the right MCA (M1Rt) in male and female patients with stroke [Table 3] was significantly different (P < 0.05).
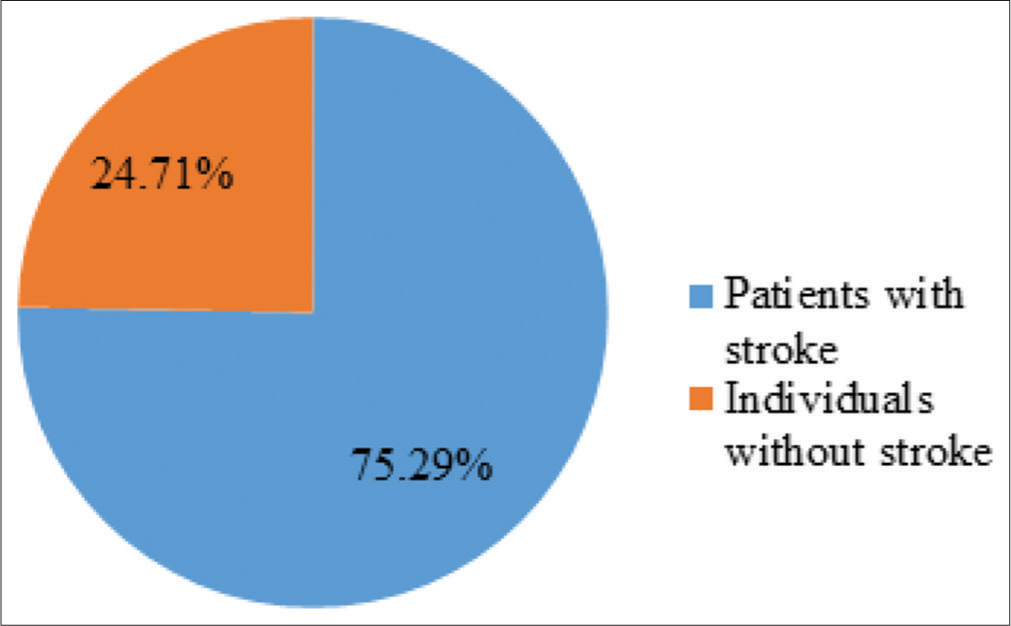
- Pie chart distribution of the total sampled images.

- Magnetic resonance imaging angiogram of the circle of Willis in individuals without stroke.

- Axial computed tomography maximum intensity projection angiogram of the circle of Willis in individuals without stroke.

- Volume rendered image of circle of Willis in patients with stroke.
| Artery | Individuals without stroke | Patients with stroke | ||
|---|---|---|---|---|
| Male (n=52) |
Female (n=32) |
Male (n=152) |
Female (n=104) |
|
| A1Lt | 1.62±0.05 | 1.50±0.04 | 1.52±0.05 | 1.29±0.04* |
| M1Rt | 2.11±0.05 | 1.82±0.05 | 4.36±0.06* | 3.18±0.06* |
| M1Lt | 2.01±0.06 | 1.69±0.05 | 1.49±0.06 | 1.03±0.05* |
| P1Rt | 1.85±0.05 | 1.51±0.05 | 2.72±0.05 | 1.92±0.04* |
| P1Lt | 1.71±0.04 | 1.43±0.05 | 1.11±0.04 | 1.08±0.03* |
| BA | 2.09±0.05 | 1.86±0.05 | 3.60 | 2.15 |
Values expressed as mean±SEM, *Significantly different at P<0.05
DISCUSSION
In our study, the luminal diameter of major arteries that form the circle of Willis measured in male and female individuals without stroke ranged from 1 mm to 2.11 mm. In this case, the individuals without stroke were considered apparently normal with no significant difference noted in luminal diameter of the pre-communicating part of the ACA (A1), the sphenoidal part of the MCA (M1), the first portion of PCA (P1), and the BA portion that also form the circle of Willis (P < 0.05). Result of the present study is in tandem with similar work on vascular luminal diameter of the circle of Willis that ranged from 1 mm to 3 mm specific to TOF MRI angiography in a sampled Indian population.[8] In addition, our findings support works in which arteries of the circle of Willis measured with methods such as the cadaveric gross dissection, injection technique, and advanced imaging modalities including CTA and MRI scans to establish normal vascular luminal dimensions in male and female individuals that ranged from 1 mm to 3 mm in their sampled populations.[15-22] The luminal diameters obtained from this study may, therefore, be reference values specific to CTA and MRI circle of Willis. Deviation from these values noted may be helpful in the identification/pattern recognition of vessel(s) and structures in the brain of individuals affected with stroke.
On comparison, it was observed that patients (male and female) with stoke had larger luminal diameter of major arteries that form the circle of Willis. This ranged from 1 mm to > 3 mm (P < 0.05). The larger luminal diameters noted in the present study in patients with stroke may be associated with the presence of either a plaque-encrusted artery that has lost its elasticity to become brittle, thin, prone to cracking and eventually breaks up or a bleeding ruptured aneurysm including cerebral arteriovenous malformation, vascular risk factors, and comorbidities associated with stroke. These defective blood vessels, when subjected to abnormal pressure or damage, affect the arterial supply to the brain.[27] Therefore, the aforementioned factors may have predisposed patients with stroke observed in this study to having larger luminal diameter because of the increased pressure in the anastomotic arterial supply that attempts to compensate for the blocked/ruptured vessel, causing vascular inefficiency with attendant secondary consequences. Result of the present study corroborates works that observed larger luminal diameter of arteries of the circle of Willis.[22,23] In addition, our findings support similar work that recorded larger luminal diameter of the ACA on MRI angiograms in males.[16]
The use of advanced imaging modalities such as the CTA and MRI in the present study is very important as the CTA and MRI scans have the potential to provide significant information about features of stroke that may guide the management of patients affected. The study has established for the 1st time an index, specific to CTA and MRI luminal diameters of the circle of Willis in a sampled Nigerian population. In view of this, the reference provided may be of diagnostic value and useful/helpful in investigating other pathology of the circle of Willis and the entire brain. In addition, the anatomic imaging parameters of the circle of Willis obtained may be useful in the construction of angiographic microcatheters used in endovascular techniques. Therefore, results of this study may be applied in the proper management and possible treatment of patients affected with ischemic stroke.
CONCLUSION
Patients with stroke have larger luminal diameter of major arteries that form the circle of Willis. This ranged from 1 mm to >3 mm when compared to patients without stroke whose luminal diameter ranged from 1 mm to 2.11 mm. However, the use of CTA and MRI in the present study cannot be overemphasized.
Acknowledgments
The authors acknowledged the Federal Health Research Ethics Committee, FCT, Abuja, for the ethical approval/ clearance of the study. Also, the Management and Staff of the Jos University Teaching Hospital, Jos, the Asi Ukpo Hospital Calabar, the Intercontinental Diagnostics Centre GRA Port Harcourt, the Afriglobal Medicare Limited, Lagos, the National Hospital and the e-Clinic and Diagnostic Limited, Abuja, will always be remembered for the permission granted to use the images obtained from their CT and MRI scanners for the present study.
Declaration of patient consent
Patient’s consent not required as patient’s identity was not disclosed or compromised in the study.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Vascular supply of the brain In: Gray's Anatomy, ed. The Anatomical Basis of Clinical Practice (40th ed). Edinburg: Elsevier Churchill Living Stone; 2008.
- [Google Scholar]
- Dr. Thomas Willis' famous eponym: The circle of Willis. Turk J Med Sci. 2004;34:271-4.
- [Google Scholar]
- Evaluation of anatomical variants of the circle of Willis in a Nigerian population using contrast enhanced computed tomography (CECT) scan. Int J Sci Eng Res. 2017;8:2129-35.
- [Google Scholar]
- Anatomical variations of the circulus arteriosus in cadaveric human brains. Neurol Res Int. 2014;2014:687281.
- [CrossRef] [PubMed] [Google Scholar]
- Classical pattern of the cerebral arterial circle of Willis in a Nigerian population using contrast enhanced computed tomography scan. Int J Sci Eng Res. 2017;8:1204-7.
- [Google Scholar]
- The blood supply of the brain and spinal cord In: Clinical Neuroanatomy (7th ed). New Delhi, India: Wolters Kluwer Pvt. Ltd.; 2010.
- [Google Scholar]
- Blood supply of the brain In: Textbook of Clinical Neuroanatomy (2nd ed). Amsterdam, Netherlands: Elsevier Health Science; 2014.
- [Google Scholar]
- Diameter of anterior cerebral artery on MRI angiograms. Int J Anat Res. 2016;4:2245-50.
- [CrossRef] [Google Scholar]
- Variation in form of circle of Willis: Some anatomical and embryological considerations. Anat Res. 1976;185:119-23.
- [CrossRef] [PubMed] [Google Scholar]
- Admission hyperglycaemia and cerebral perfusion deficits in acute ischaemic stroke. Cerebrovasc Dis. 2013;35:163-7.
- [CrossRef] [PubMed] [Google Scholar]
- Heart disease and stroke statistics-2014 update: A report from the American Heart Association. Circulation. 2014;129:228-92.
- [Google Scholar]
- Measuring elevated microvascular permeability and predicting hemorrhagic transformation in acute ischemic stroke using first-pass dynamic perfusion CT imaging. BMC Neurol. 2014;14:6-8.
- [Google Scholar]
- Preventing stroke: Saving lives around the world. Lancet Neurol. 2007;6:182-7.
- [CrossRef] [Google Scholar]
- How complex interactions of ischemic brain infarcts, white matter lesions, and atrophy relate to poststroke dementia. Arch Neurol. 2000;57:1295-300.
- [CrossRef] [PubMed] [Google Scholar]
- Dimensions of the circle of Willis and dynamic studies using electrical analogy. J Neurosurg. 1964;21:26-34.
- [CrossRef] [PubMed] [Google Scholar]
- Circle of Willis: Morphologic variation on three-dimensional time-of-flight MR angiograms. Radiology. 1998;207:103-11.
- [CrossRef] [PubMed] [Google Scholar]
- Blood vessel size of circulus arteriosus cerebri (circle of Willis): A statistical research on 100 human subjects. J Anat. 1985;123:72-6.
- [CrossRef] [PubMed] [Google Scholar]
- Observations on the length and diameter of vessels forming the circle of Willis. J Anat. 1981;133:419-23.
- [Google Scholar]
- Microsurgical anatomy of the anterior cerebral artery-anterior communicating artery complex: An Indian study. Neurol Asia. 2005;10:21-8.
- [Google Scholar]
- Biometrical aspects of the anterior cerebral artery in its proximal segment (A1) and internal carotid artery. Int J Morphol. 2007;25:915-8.
- [CrossRef] [Google Scholar]
- Variations in the configuration of the circle of Willis. Anat Sci Int. 2008;83:98-106.
- [CrossRef] [PubMed] [Google Scholar]
- Measurement of diameter of blood vessels forming circle of Willis and their variations by magnetic resonance imaging angiography. J Anat Soc India. 2008;57:53-9.
- [Google Scholar]
- Comparison of perfusion computed tomography and computed tomography angiography source images with perfusion-weighted imaging and diffusion-weighted imaging in-patients with acute stroke of less than 6 hours' duration. Stroke. 2004;35:1652-8.
- [CrossRef] [PubMed] [Google Scholar]
- Perfusion-CT assessment of infarct core and penumbra: Receiver operating characteristic curve analysis in 130 patients suspected of acute hemispheric stroke. Stroke. 2006;37:979-85.
- [CrossRef] [PubMed] [Google Scholar]
- Outcomes in mild or rapidly improving stroke not treated with intravenous recombinant tissue-type plasminogen activator. Stroke. 2011;42:3110-5.
- [CrossRef] [PubMed] [Google Scholar]
- CT and MRI early vessel signs reflect clot composition in acute stroke. Stroke. 2011;42:1237-43.
- [CrossRef] [PubMed] [Google Scholar]




