
Translate this page into:
Burden of nosocomial tuberculosis and effect of educational intervention on infection prevention and control among healthcare workers in Kaduna state northwest, Nigeria

*Corresponding author: Chiroma Laminu, Department of Public Health, Lead City University, Ibadan, Nigeria. chiromalaminu22@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Laminu C. Burden of nosocomial tuberculosis and effect of educational intervention on infection prevention and control among healthcare workers in Kaduna state northwest, Nigeria. Calabar J Health Sci 2023;7:84-92. doi: 10.25259/CJHS_4_2024
Abstract
Objectives:
Tuberculosis (TB) is one of the top ten leading causes of death from a single pathogen, caused by Mycobacterium tuberculosis (MTB) affecting the lungs and other parts of the body, pulmonary TB and extrapulmonary TB. TB is the increased rate of transmission among healthcare workers (HCWs), especially in developing nations, due to resource constrained. The study assessed the burden of nosocomial TB and the effect of educational intervention on infection prevention and control among HCWs in Kaduna State.
Material and methods:
Records of health facilities offering TB services were reviewed and cross-sectional survey designs were used to obtain pre- and post-intervention data from health workers for this study. All healthcare personnel providing TB care services in healthcare facilities across Kaduna State were included in the study population. A multi-stage purposive sampling procedure was adopted for the selection of the healthcare facilities. The educational intervention using World Health Organization guidelines on TBIC was provided among HCWs. The HCW’s knowledge of TBIC was assessed post-intervention. However, post-intervention was also conducted after 6 months to determine the effect of the training intervention. Data were collected using a checklist to determine the case fatality and incidence rate of TB. An adopted questionnaire was used to assess the level of knowledge on TBIC among HCWS during pre- and post-intervention. Descriptive statistics and t-tests were used to analyze the data (x = 0.05).
Results:
The incidence and case fatality due to TB among HCWs in Kaduna State was 0.158% and 30%, respectively. The effect of the educational intervention was statistically significant at (0.001). Despite the low incidence of TB among HCWs, the case fatality is high among this cohort.
Conclusion:
However, educational intervention in TB infection prevention and control is effective in reducing nosocomial TB among HCWs. A prospective cohort study is recommended to document the actual TB burden among HCWs in the state.
Keywords
Nosocomial transmission
Burden of tuberculosis
Healthcare workers

INTRODUCTION
Nosocomial tuberculosis (TB) has been reported in sub-Saharan Africa to result in significant morbidity and mortality in patients and healthcare workers (HCWs) due to poor provision and implementation of TB infectious control.[1] HCWs remained susceptible to developing TB despite the decline of the disease in the general population.[2] The transmission of occupational TB is on the increase among nations with limited resources and a high burden of TB/human immunodeficiency virus (HIV). The median annual incidence of occupationally acquired TB was 5.8% in low-income countries compared to 1.1% in high-income countries due to poor implementation of the World Health Organization (WHO) guidelines on infection prevention and control.[3] The attributable risk for TB disease in HCWs, compared to the risk in the general population, ranged from 25 to 5361/100 000 per year.[4] Carelessness of health professionals to seek medical attention, poor working environment, inadequate personal protective equipment, fear of discrimination, inconsistent supervision and surveillance, medical conditions such as cancer and diabetes mellitus, and other risky lifestyles like alcoholism increase the associated risk factors for developing active TB among frontline HCWs globally.[5] It documented that DOT’s centers are widely available across Kaduna State, this implies that a significant number of HCWs were exposed to developing nosocomial TB if not adequately trained on TBIC using WHO guidelines.[6]
Insufficient training on tuberculosis infection prevention and control (TBIPC) is the documented reason that determined the high TB rate among HCWs in the developing world.[7] Due to the importance of training HCWs on TBIC in reducing the burden of nosocomial TB, the training has been made the general responsibility of public and private organizations.[8] It is recommended that educating health professionals in the prevention and control of infection should be made periodic to ensure implementation and updated knowledge of these guidelines.[9] The lack of comprehensive reports on the incidence of active TB among HCWs in Nigeria is a documented reason for increasing the transmission of occupational TB among these cohorts in the Country.[10] Infected HCWs should be encouraged to repotting themselves for the effective treatment of TB using the WHO End-TB strategy.[11] The study is aimed to assess the burden of nosocomial TB and the effect of educational training among HCWs in Kaduna State, Nigeria.
MATERIAL AND METHODS
Study design
Records of Health facilities offering TB services were reviewed from 2006 to 2020, and cross-sectional survey designs were used to obtain pre- and post-intervention data from health workers for this study [Annexure 1].
| Item No | Recommendation | PageNo | |
|---|---|---|---|
| Title and abstract | 1 | (a) Indicate the study’s design with a commonly used term in the title or the abstract | 1–2 |
| (b) Provide in the abstract an informative and balanced summary of what was done and what was found | |||
| Introduction | |||
| Background/rationale | 2 | Explain the scientific background and rationale for the investigation being reported | 3–4 |
| Objectives | 3 | State specific objectives, including any prespecified hypotheses | 4 |
| Methods | |||
| Study design | 4 | Present key elements of study design early in the paper | 4 |
| Setting | 5 | Describe the setting, locations, and relevant dates, including periods of recruitment, exposure, follow-up, and data collection | 4 |
| Participants | 6 | (a) Give the eligibility criteria, and the sources and methods of selection of participants | 4 |
| Variables | 7 | Clearly define all outcomes, exposures, predictors, potential confounders, and effect modifiers. Give diagnostic criteria, if applicable | 4 |
| Data sources/measurement | 8* | For each variable of interest, give sources of data and details of methods of assessment (measurement). Describe comparability of assessment methods if there is more than one group | 4–5 |
| Bias | 9 | Describe any efforts to address potential sources of bias | |
| Study size | 10 | Explain how the study size was arrived at | 5 |
| Quantitative variables | 11 | Explain how quantitative variables were handled in the analyses. If applicable, describe which groupings were chosen and why | |
| Statistical methods | 12 | (a) Describe all statistical methods, including those used to control for confounding | 5 |
| (b) Describe any methods used to examine subgroups and interactions | |||
| (c) Explain how missing data were addressed | |||
| (d) If applicable, describe analytical methods taking account of sampling strategy | |||
| (e) Describe any sensitivity analyses | |||
| Results | |||
| Participants | 13* | (a) Report numbers of individuals at each stage of study - for example, numbers potentially eligible, examined for eligibility, confirmed eligible, included in the study, completing follow-up, and analyzed | 5 |
| (b) Give reasons for non-participation at each stage | 5 | ||
| (c) Consider use of a flow diagram | |||
| Descriptive data | 14* | (a) Give characteristics of study participants (e.g., demographic, clinical, and social) and information on exposures and potential confounders | |
| (b) Indicate number of participants with missing data for each variable of interest | |||
| Outcome data | 15* | Report numbers of outcome events or summary measures | |
| Main results | 16 | (a) Give unadjusted estimates and, if applicable, confounder-adjusted estimates and theirprecision(e.g.,95%confidenceinterval).Makeclearwhichconfounderswere adjusted for and why they were included | 6 |
| (b) Report category boundaries when continuous variables were categorized | |||
| (c) If relevant, consider translating estimates of relative risk into absolute risk for a meaningful time period | |||
| Other analyses | 17 | Reportotheranalysesdone–forexample,analysesofsubgroupsandinteractions,and sensitivity analyses | |
| Discussion | |||
| Key results | 18 | summarize key results with reference to study objectives | 7 |
| Limitations | 19 | Discuss limitations of the study, taking into account sources of potential bias or imprecision. Discuss both direction and magnitude of any potential bias | 10 |
| Interpretation | 20 | Give a cautious overall interpretation of results considering objectives, limitations, multiplicity of analyses, results from similar studies, and other relevant evidence | 10 |
| Generalizability | 21 | Discuss the generalizability (external validity) of the study results | 11 |
| Other information | |||
| Funding | 22 | Give the source of funding and the role of the funders for the present study and, if applicable, for the original study on which the present article is based | 12 |
Population of the study
Medical personnel, pharmacies, health records officers, community health, environmental health, X-ray technicians, and medical laboratories that provide TB treatment services through DOTs from both public and commercial facilities in Kaduna State are included in the study population.
Study area
Kaduna State, which occupies 46,053 km2 overall, is situated in Nigeria’s northwest geopolitical zone. The state’s population is expected to be 8,397,541 throughout its 23 local government area (LGA) in 2017, up 3.0% from the 6,113,503 national predictions from 2006 ( National Bureau of Statistics [NBS], 2017). Agricultural activities are the major source of income in the state. Six LGAs were selected for the conduct of this study, including Kubau and Zaria from Zone A, Igabi and Kaduna North from zone B, and Kauru and Kachia were also selected from zone C, respectively. However, 36 health facilities were also selected, six from each of the selected LGA.
Data source
Primary data were collected from HCWs using a questionnaire to assess the HCW’s level of knowledge on TBIC at pre- and post-intervention from the health facilities, educational intervention was provided among HCWs using the WHO guidelines on TBIC, and the secondary data were collected using a checklist from the TB central register to determine TB burden.
Study size
The study was conducted among 36 healthcare facilities providing TB care services in Kaduna State, Nigeria.
Sample size determination
An appropriate sample size was calculated based on the following assumptions:
27.8% prevalence of TB among HCWs, this was adopted from South
Africa due to the low prevalence of TB among HCWs in Nigeria. The sample size was determined using the Yamane formula for sample size determination.
Where,
Z = 1.96.
P = 0.278 (27.8% prevalence).
e = 0.05 (precision rate).
n = 306.
+ 10% non-response rate = 31.
306 + 31 = 339.
n = 339.
Sampling methods
A multistage purposive sampling procedure was used. The first stage stratified the state according to the three senatorial districts. The second stage selected 36 health facilities, both public and private, from six (6) selected local governments and two (02) LGAs per senatorial district, considering urban and rural characteristics using purposive sampling. The third stage has purposively selected 339 HCWs working at the DOT’s clinic.[2]
Data collection
Data were collected using a checklist on the record of TB among HCWs from 2006 to 2020 across the 36 health facilities to determine incidence and case fatality rates. However, to provide educational intervention, a training tool was adopted from the WHO guideline on TBIC. Data were also collected using a questionnaire during pre- and post-intervention to determine the significance of the training intervention after 6 months. Other data on the provision and implementation of TBIC were also collected using a questionnaire.
Data analysis
Secondary data collected from the TB central register using a checklist were analyzed using an epidemiological formula to determine incidence and case fatality rate, and the result was presented in proportion/percentage. All data collected on the effect of educational intervention were cleaned and entered into the statistical package of social science software version 23.0. The sociodemographics of the respondents and other factors that were nominal data were presented as counts and percentages. Paired t-test was used to compare the difference between the pre- and post-intervention knowledge and practices. The chi-square test was used to determine the level of statistical significance and drivers of the knowledge of TBIC.
Ethical clearance
Ethical clearance/approval was obtained from the Kaduna State Ministry of Health Research Committee, Health Research and Ethical Committee, National TB and leprosy training center Zaria and Lead City University Research Ethical Committee (LCU/REC/22/103). The study has no harm on the participants. The participants were informed of their willingness and right to participate or withdraw from the study. The participants benefited from the free educational training provided by this study.
RESULTS
Demographic characteristics of respondents
A total of 325 respondents were interviewed, out of which 171 (52.6%) were male 175 (53.8%) were between the ages of 25 and 34, with a mean age of 31.51 ± 8.24. Among these health workers, 220 (67.7%) are married, 158 (48.6%) have National certification examination (NSE)/Ordinary nationa diploma (OND) degrees, 136 (41.1%) have higher degrees and only 31 (9.5%) have a secondary school certificate and below. More than 50% of the respondents were either laboratory personnel 93 (28.7%) or community HCWs 87 (26.8%). The result of this analysis also shows that the majority of the respondents were community health workers, 87 (26.8%), while only 21 (6.5%) were doctors, respectively. About 36.6% of the respondents were from the general outpatient department, while 46 (14.2%) were from the DOTS centre [Table 1]. The majority of the respondents, 51.4%, were from urban settings, while 48.6% were from rural healthcare facilities [Table 1].
| Variable | Frequency | Percent |
|---|---|---|
| Age group | ||
| Mean age (±SD) | 31.51±8.24 | |
| 24andbelow | 49 | 15.1 |
| 25–34 | 175 | 53.8 |
| 35–44 | 71 | 21.8 |
| 45 and above | 30 | 9.2 |
| Sex | ||
| Male | 171 | 52.6 |
| Female | 154 | 47.4 |
| Marital status | ||
| Single | 96 | 29.5 |
| Married | 220 | 67.7 |
| Others | 9 | 2.8 |
| Education qualification | ||
| Secondary and below | 31 | 9.5 |
| OND/NCE | 158 | 48.6 |
| Higher | 136 | 41.8 |
| Cadre | ||
| Doctors | 21 | 6.5 |
| Nurse | 59 | 18.2 |
| Laboratory personnel | 93 | 28.7 |
| Community health | 87 | 26.8 |
| Environmental | 30 | 9.2 |
| Medical records | 25 | 7.7 |
| Health attendant | 35 | 10.8 |
| Unit | ||
| GOPD | 119 | 36.6 |
| Laboratory | 43 | 13.2 |
| DOTs | 46 | 14.2 |
| Record | 25 | 7.7 |
| Ward | 55 | 16.9 |
| Others | 37 | 11.4 |
| Facility setting | ||
| Urban | 51.4 | |
| Rural | 48.6 |
Source:Researcher’sSurvey(2022).SD:Standarddeviation,OND:Ordinarynational diploma, NCE: National certification examination, GOPD: General outpatients department, DOTs: Directly observed therapies.
The result of the analysis shows that 6325 TB cases were documented among the general population from 2006 to 2020, 5811 were declared cured, 481 were satisfied death, 33 were lost to follow-up, 362 were TB/HIV co-infected, 10 cases were reported among HCWs, two cases were TB/HIV co-infected among TB in HCWs, seven were declared cured, and three cases were satisfied death [Table 2].
| Total number of confirm TB case | 6325 |
| Cured | 5811 |
| Death | 481 |
| Lost to follow-up | 33 |
| TB/HIV Co-infection | 362 |
| TB in HCWs | 10 |
| TB/HIV in HCWs | 2 |
| TB Cured in HCWs | 7 |
| TB Death in HCWs | 3 |
Source: Researcher’s survey (2022). TB: Tuberculosis, HIV: Human immunodeficiency virus, HCWs: Healthcare workers
This result shows that 6325 active cases were diagnosed among general populations, including HCWs, from 2006 to 2020, out of which 5811 were declared cured, 481 were satisfied with death, and 33 were lost to follow-up. Out of the 6325 cases, only 10 (0.16%) were HCWs, out of which 2 (20%) cases were TB/HIV co-infection, 7 (70%) were declared cured, and three were satisfied cured [Figure 1].
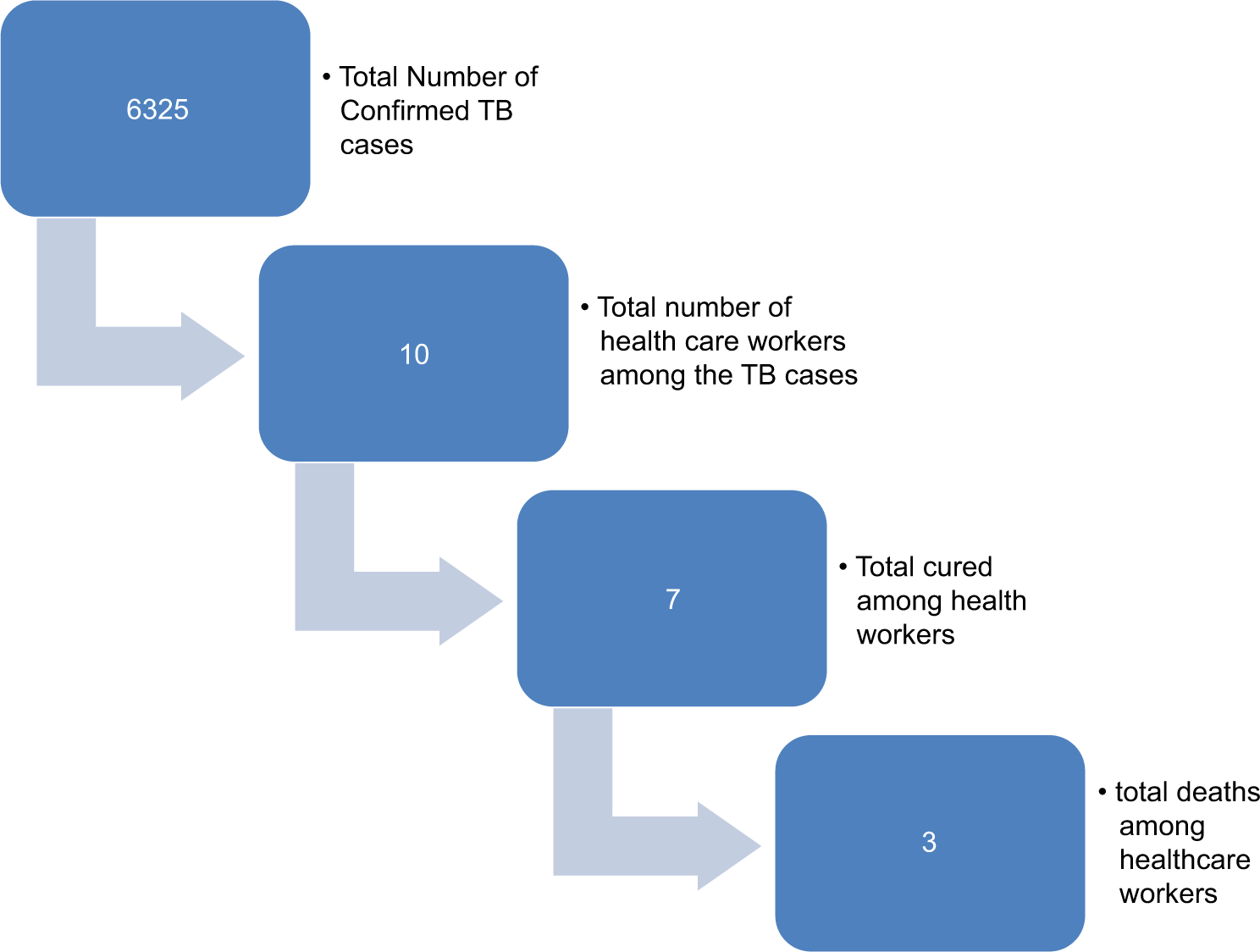
- Confirm tuberculosis (TB) cases among general populations. Source: Researcher’s survey (2022).
The overall result of this analysis shows that only 6% and 22% have good implementation and adequate provision of TB infection prevention and control [Figure 2].
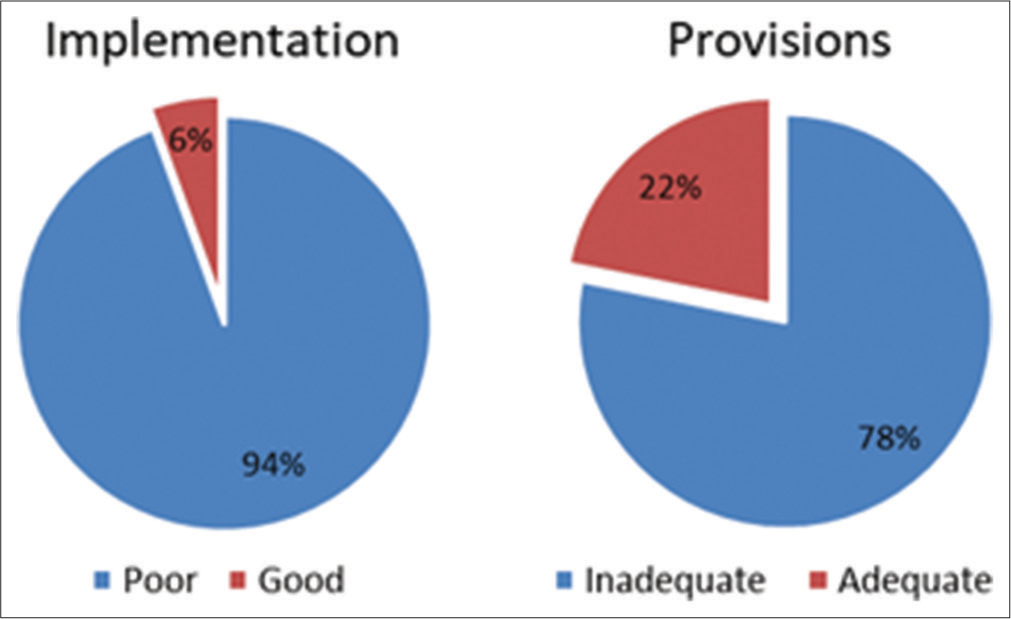
- Provision and implementation of World Health Organization guideline on tuberculosis infectious control. Source: Researcher’s survey (2022).
The result of this analysis shows that only 29.8% have good knowledge of TB infection prevention and control during pre-intervention, while 70.2% have good knowledge at post-intervention [Chart 1].
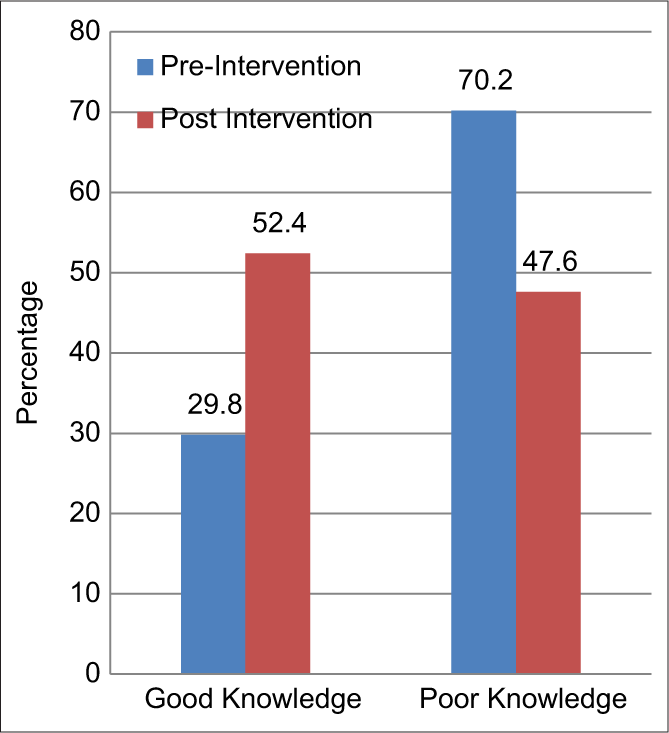
- Knowledge of tuberculosis infection control (pre and post intervention scores). Source: Researcher’s survey (2022).
DISCUSSION
The study findings revealed that among HCWs in Kaduna State, only ten out of the 6325 confirmed cases of TB were reported as active TB cases. This suggests that the incidence rate of TB among HCWs in the state is approximately 0.158%. The study’s results are in line with similar research conducted in Egypt, which reported a 0.5% prevalence of TB among HCWs.[12] In addition, a separate study conducted in Uganda documented a prevalence rate of 1.7% of TB among HCWs.[13] Ethiopia reported a prevalence rate of 1.4%.[14] Another study in Nigeria has reported a 1.5% prevalence of active TB among HCWs.[15] Furthermore, a study in Nigeria documented different incidence rates of TB among HCWs, with rates of 3.3% and 2.2% reported by acid-fast bacilli and culture methods, respectively.[1] In Zambia, a study reported a prevalence of 38.3% of active TB among bedside contacts.[16] In South Africa, a significant prevalence of 27.8% of TB was reported among HCWs.[17] These variations in prevalence and incidence rates can be attributed to differences in study design, such as prospective cohort studies, as well as differences in the reporting systems for TB cases among HCWs across Egypt, Ethiopia, Uganda, and Nigeria. In a recent study conducted in Kaduna State, Nigeria, a prevalence of 0.158% of active TB among HCWs was reported, aligning with the earlier finding.[18]
Among HCWs, ten cases of TB were confirmed; out of these, three individuals were declared dead, implying a case fatality rate of 30% due to TB in this cohort. This high case fatality rate was likely due to the prevalent HIV infection among the HCWs. This finding is consistent with a study conducted in Malawi, which reported an overall case fatality rate of 24% due to TB among HCWs.[19] Another study in South Africa documented a 13% death rate due to TB among HCWs.[20] In contrast, a study in Nigeria reported a lower death rate of 6.3% due to TB among HCWs.[1] Furthermore, two studies, one in South Africa and another in Taiwan, both reported 0% death rates from TB in HCWs.[21,22] The differences in TB-related mortality among HCWs across these studies can be attributed to the presence or absence of HIV co-infection. A recently published study documented 30% of deaths due to TB among HCWs in Kaduna State.[18]
The results of this study indicated that the provision and implementation of the WHO guidelines on TB infection prevention and control (TB IPC) was insufficient. This finding is similar to a study in Mozambique that reported inadequate implementation of infection control measures due to a lack of clear training on the TB IPC guidelines.[23] Likewise, a study in South Africa found poor implementation of TB IPC practices due to a lack of training.[24] Another study conducted in Ethiopia attributed the lack of proper TB IPC practices to insufficient infrastructure and resources. A systematic review also documented that the provision and implementation of TB IPC measures are frequently inadequate across various settings.[25] Another study identified poor implementation of TB IPC measures in health settings in Bangladesh.[26] It is documented from a study that only less than half of the HCWs had good practices of TB infection control;[27] it is also reported from a study that the proportion of proper TBIPC practices among public HCWs was low.[28] Another study in Lagos, Nigeria, documented poor provision of TB infection control equipment.[29] Consistent with these findings, a recent study in Kaduna state, Nigeria, also reported insufficient provision and implementation of the WHO guidelines on TB infection prevention and control.[2]
The results of this study show that the training interventions provided on the WHO guidelines for TB infection control were statistically significant when comparing the pre-intervention and post-intervention overall scores. This finding is in line with a study that reported improvement in post-intervention scores, implying that the educational intervention adopted for this study was effective in improving TBIC among the nurses.[30] Similarly, another study found that the training intervention led to improved knowledge of symptoms, prevention, diagnosis, and treatment of TB among community health workers.[31] Additional studies documented that educational interventions increased staff knowledge of TB infection prevention and control and that such interventions are significant in preventing TB transmission among HCWs.[32] Another study reported that educational intervention is significant in preventing TB among HCWs.[33] Consistent with these findings, a recent study conducted in Kaduna state, Nigeria, identified that providing educational training on TB infection control using the WHO guidelines is an effective way to reduce nosocomial (hospital-acquired) TB.[34,35]
Decision rule
If the P-value is greater than the critical value (0.05), we fail to accept the null hypothesis; hence, otherwise. Since the majority of the P-value satisfies otherwise (i.e., <0.005), then the decision rule is to reject the null hypothesis (H0), which states that there is a significant difference between the pre and post-test.
Limitations of the study
The limitations of this research study include challenges with data quality and poor/improper documentation of confirmed TB cases among HCWs. The educational intervention was provided at each senatorial district due to the inability to gather all the participants at the same venue as the result of distance and fear of insecurity.
Interpretation
Despite the high fatality rate due to TB among healthcare workers, the incidence rate remained low due to poor documentation in Kaduna State. The provision of educational intervention on TBIC using the WHO guideline is an effective way to reduce nosocomial TB among HCWs.
Recommendation
Educational training and retraining of HCWs on WHO TBIC should be provided to all HCWs providing TB care services through DOTs. Records of active TB cases in HCWs should be properly documented so as to document the actual TB burden among HCWS. The provision and implementation of TBIC guidelines should be adequately provided across all health facilities providing TB care services.
CONCLUSION
Providing adequate educational training intervention is a way to reducing the burden of tuberculosis among healthcare workers in Kaduna State, Nigeria.
Acknowledgments
We acknowledge the nurses, doctors, health record officers, community health, and all allied health professionals in Kaduna state, Nigeria, for their cooperation in data collection. We also thank the staff of the Research and Ethics Committee of Kaduna State Ministry of Health, Nigeria and the National Tuberculosis and Leprosy Training Center Zaria, Kaduna State, Nigeria, for assisting in securing the ethical approval to conduct the study.
Ethical approval
The authors declare that they have taken the Institutional Ethical Committee approval and the approval number is LCU/REC/22/103.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Pulmonary tuberculosis among health care workers at two designated DOTS Centers in urban city of Ibadan, Nigeria. Indian J Med Res. 2011;133:613-7.
- [Google Scholar]
- Implementation of WHO guideline on tuberculosis infection prevention and control in Kaduna State, Nigeria. PAMJ One Health. 2023;12:1.
- [CrossRef] [Google Scholar]
- Risk of prevalence of latent tuberculosis infection in health care workers-an idiographic meta-analysis from a Chinese perspective. J Thorac Dis. 2021;13:2378-92.
- [CrossRef] [PubMed] [Google Scholar]
- Implications of asymptomatic carriers for tuberculosis transmission and control in Thailand: A modelling approach. 2024
- [CrossRef] [Google Scholar]
- Burdens of infection control on healthcare workers: A scoping review. J Hosp Infect. 2024;146:76-81.
- [CrossRef] [PubMed] [Google Scholar]
- An assessment of primary health care costs and resource requirements in Kaduna and Kano, Nigeria. Front Public Health. 2023;11:1226145.
- [CrossRef] [PubMed] [Google Scholar]
- Reducing the risk of tuberculosis transmission for HCWs in high incidence settings. Antimicrob Resist Infect Control. 2021;10:106.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence and risk factors for Mycobacterium tuberculosis infection among health workers in HIV treatment centers in North Central, Nigeria. Am J Trop Med Hyg. 2023;109:60-8.
- [CrossRef] [PubMed] [Google Scholar]
- Knowledge, attitudes and preventive practices regarding tuberculosis among healthcare workers and patients in India: A mixed-method study. Cureus. 2024;16:e56368.
- [CrossRef] [PubMed] [Google Scholar]
- Investigating socio-ecological factors influencing implementation of tuberculosis infection prevention and control in rural Papua New Guinea. J Public Health. 2024;46:267-76.
- [CrossRef] [PubMed] [Google Scholar]
- The prevalence and risk factors for tuberculosis among healthcare workers in Yogyakarta, Indonesia. PLos One. 2023;18:e0279215.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence of tuberculosis among healthcare workers in Cairo University Hospitals. Egypt J Occup Med. 2015;39:213-30.
- [CrossRef] [Google Scholar]
- Tuberculosis infection among health care workers in Kampala, Uganda. Int J Tuberc Lung Dis. 2005;9:686-8.
- [Google Scholar]
- Prevalence of active tuberculosis disease among healthcare workers and support staff in healthcare settings of the Amhara region, Ethiopia. PLoS One. 2021;16:e0253177.
- [CrossRef] [PubMed] [Google Scholar]
- Tuberculosis among the health-care workers of the University of Ilorin Teaching Hospital. Trop Doct. 2007;37:251.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence of tuberculosis among bedside contacts of smear positive tuberculosis patients at the university teaching hospital, Lusaka, Zambia. Med J Zambia. 2020;47:170-8.
- [CrossRef] [Google Scholar]
- The epidemiology of tuberculosis in health care workers in South Africa: A systematic review. BMC Health Serv Res. 2016;16:416.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence of occupational tuberculosis among healthcare workers in Kaduna State, Nigeria. PAMJ One Health. 2023;12:2.
- [Google Scholar]
- Tuberculosis in health care workers in Malawi. Trans R Soc Trop Med Hyg. 1999;93:32-5.
- [CrossRef] [PubMed] [Google Scholar]
- High incidence of hospital admissions with multidrug-resistant and extensively drug-resistant tuberculosis among South African health care workers. Ann Intern Med. 2010;153:516-22.
- [CrossRef] [PubMed] [Google Scholar]
- The treatment outcomes of tuberculosis among health care workers in a general hospital in the Mpumalanga province, South Africa. Afr J Prim Health Care Family Med. 2009;1:86.
- [CrossRef] [Google Scholar]
- Tuberculosis in healthcare workers: A matched cohort study in Taiwan. PLoS One. 2015;10:e0145047.
- [CrossRef] [PubMed] [Google Scholar]
- Healthcare workers' challenges in the implementation of tuberculosis infection prevention and control measures in Mozambique. PLoS One. 2014;9:e114364.
- [CrossRef] [PubMed] [Google Scholar]
- Barriers to the implementation of tuberculosis infection control among South African healthcare workers. South Afr Health Rev. 2012;2012:197-203.
- [Google Scholar]
- Barriers and facilitators of tuberculosis infection prevention and control in low-and middle-income countries from the perspective of healthcare workers: A systematic review. PLoS One. 2020;15:e0241039.
- [CrossRef] [PubMed] [Google Scholar]
- Health worker experiences of implementing TB infection prevention and control: A qualitative evidence synthesis to inform implementation recommendations. PLOS Glob Public Health. 2022;2:e0000292.
- [CrossRef] [PubMed] [Google Scholar]
- Exploring the role of healthcare personnel in designing tuberculosis infection prevention and control measures in healthcare settings: A scoping review. Int J Environ Res Public Health. 2024;21:524.
- [CrossRef] [PubMed] [Google Scholar]
- Implementation status of national tuberculosis infection control guidelines in Bangladeshi hospitals. PLoS One. 2021;16:e0246923.
- [CrossRef] [PubMed] [Google Scholar]
- Tuberculosis infection control practice and associated factors among health care workers in Ethiopia: Systematic review and meta-analysis. PLos One. 2023;18:e0295555.
- [CrossRef] [PubMed] [Google Scholar]
- The effect of an educational intervention to improve tuberculosis infection control among nurses in Ibadan, south-west Nigeria: A quasi-experimental study. BMC Nurs. 2020;19:81.
- [CrossRef] [PubMed] [Google Scholar]
- Effect of training of frontline health workers on tuberculosis: A cluster randomized control trial in South Nigeria. F1000Research. 2022;10:837.
- [CrossRef] [Google Scholar]
- Evaluation of the impact of an educational intervention aimed at improving tuberculosis infection control knowledge among health care workers in a military treatment facility: A quality improvement project United States: West Virginia University; 2020.
- [Google Scholar]
- Effectiveness of health education intervention in improving knowledge, attitude, and practices regarding tuberculosis among nurses working in tuberculosis centers in Libya. AlQalam J Med Appl Sci. 2023;6:230-9.
- [Google Scholar]
- Assessment of the interventions that limits nosocomial transmission of tuberculosis among healthcare workers in Kaduna State, North-Western, Nigeria. IOSR J Nurs Health Sci. 2023;12:6-8.
- [Google Scholar]
- Educational intervention to limit occupational transmission of tuberculosis among healthcare workers in Kaduna State, Northwestern Nigeria. J Nurs Occup Health. 2024;5:558-62.
- [Google Scholar]




