
Translate this page into:
Breast cancer metastasis patterns in Yenagoa, Nigeria

*Corresponding author: Alexander Aruoriwo Dimoko, Department of Surgery, Bayelsa Medical University, Yenagoa, Bayelsa, Nigeria. zanderdimoko@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Dimoko AA, Alagoa PJ. Breast cancer metastasis patterns in Yenagoa, Nigeria. Calabar J Health Sci, doi: 10.25259/CJHS_8_2023
Abstract
Objectives:
The objective of this study was to study the characteristics and patterns of metastatic breast cancer in Yenagoa, Nigeria.
Material and Methods:
This study was a retrospective hospital-based study using a standardized data form for the capture of relevant information with definite exclusion criteria. Information gathered was captured in an Excel spreadsheet and subjected to statistical analysis. Subjects were 78 female patients diagnosed with breast cancer.
Results:
The mean age of the study population was 47.86 years. About 64% had 1–4 children while 26% had more than five children. The most common findings on general clinical examination were anemia (43.6%), cachexia (39.7%), and hepatomegaly (11.5%). On breast examination, the most common findings were axillary lymphadenopathy (87.2%), nipple changes (67.9%), peau d’orange (64.1%), skin nodules (64.1%), and chest fixity (60.3%). About 29.5% of patients had evidence of pulmonary metastasis, 19.2% had liver metastases, and 25.6% had spread to multiple sites. Central nervous system and spinal spread were found to be commoner in younger patients (<48 years).
Conclusion:
Most of the patients presenting in the hospital had evidence of metastasis. This has been found to be due mostly to delay in hospital presentation due to a complex combination of patient and healthcare-related factors. Measures for improving the dire statistics are proffered.
Keywords
Breast cancer
Metastasis
Delayed presentation
Complications
Spread pattern

INTRODUCTION
Breast cancer is the most common malignancy in women.[1,2] In 2018, over 2.09 million new cases were diagnosed worldwide resulting in more than 600,000 deaths. At least, 4.4 million women are living with breast cancer.[1,2] Age-standardized incidence rates in Nigeria range from 43.6 to 56.7/100,000 with age-standardized mortality rates of 16.7–20.0/100, 000.[1] Even in early-stage breast cancer, 20–30% of patients already have distant metastases and at least 90% of mortalities in breast cancer have been found to be due to the complications of metastatic or recurrent disease.[3,4]
This study aims to determine the sites of breast cancer metastasis in our environment to improve the allocation and deployment of resources and efficiently manage complications that are common in our area.
The most common sites for metastasis of breast cancer are the bones, liver, lungs, and brain.[3] There has been extensive research done on why these tissues are most commonly involved in distant spread. Several theories are extant and have contributed immensely to understanding this process:[4]
Growth factor theory
This holds that tumor cells in the blood or lymphatics invade organs at a similar frequency but only those that find favorable growth factors can multiply. Transferrins, for example, are iron-transferring ferroproteins needed for cell growth that have additional mitogenic properties beyond their iron-transporting functions. Increased concentrations of transferrin are found in the lungs, bone, and brain and are associated with elevated levels of transferrin receptors on metastasizing tumor cells.[5]
Adhesion theory
Endothelial cells lining the blood vessels in certain organs express adhesion molecules that bind tumor cells and allow extravasation.
Chemokine theory
Chemokines secreted by the target organ can enter the circulation and selectively attract tumor cells which express receptors for these chemokines. Breast cancer cells preferentially metastasize to the liver, bone marrow, lymph nodes, and lung. These organs secrete CXCL12-C-X-C motif chemokine 12 (CXCL12) which is the ligand for the C-X-C chemokine receptor 4 (CXCR4) which is enriched on breast cancer cells.[5]
Pre-metastatic niche theory
Bone marrow-derived progenitor cells expressing vascular endothelial growth factor (VEGF) receptor 1 and very late antigen 4 (VLA-4) are prompted by the primary tumor to establish sanctuaries for the tumor cells before their arrival.[5]
Six steps can be defined in cancer metastasis:[6,7]
Detachment: Tumor cells will detach from the primary tumor and acquire motility while losing the ability to adhere to neighboring cells
Invasion: The detached cells break through the basement membrane and migrate through surrounding tissues until they eventually reach a blood or lymphatic vessel
Intravasation: This occurs in the blood or lymphatic circulation either directly in the tumor neovasculature or indirectly in lymphatic channels
Transport and arrest
Extravasation: Migration into tissues through the vascular endothelium
Invasion of the target organ.
MATERIAL AND METHODS
Design
This study was a hospital-based retrospective study.
Setting
The study was carried out at the Federal Medical Center Yenagoa, a 400-bed hospital serving as the only tertiary health facility for the 1.2 million people of Bayelsa State.
Yenagoa is the capital of Bayelsa state with a population of approximately 250,000 people.
They are served by private clinics run by general practitioners but a lot of people patronize tradomedical practitioners, patent medicine stores, and new generation churches for their ailments.
Duration
This study duration was from January 2022 to –December 2022.
Population
All patients diagnosed with breast cancer in the hospital within the specified time period.
Study inclusion criteria
The following criteria were included in the study:
Patients with breast complaints are seen in the hospital through the general outpatient, surgical outpatient, and emergency departments
Patients who had a comprehensive history and physical examination carried out including clinical staging, laboratory investigation, and imaging
Patients who were seen or reviewed by a senior registrar or consultant
Patients with histologically confirmed breast cancer
Patients with properly documented treatment records.
Study exclusion criteria
The following criteria were excluded from the study:
Patients with incomplete and poorly documented medical records
Patients who were unable to pay for biopsy and histological analysis
Patients who were unable to carry out staging investigations such as chest X-ray, abdominal ultrasound scan, and skeletal survey.
Ninety-one patient records were retrieved but only 78 were entered in the study because 13 were ruled out by the exclusion criteria.
Methods
Patient registries in the general outpatient, surgical outpatient, and emergency departments were retrieved and examined for patients with breast-related complaints and diagnoses within the specified time period.
Patient case notes were then recovered and subjected to the inclusion and exclusion criteria listed above with a selection of patients found suitable.
Investigations carried out on these patients included:
Full blood count
Liver function tests
Excisional, incisional, or tru cut biopsy
Chest X-ray
Spinal X-rays
X-ray of long bones
Abdominal ultrasound scan.
Data analysis
Sociodemographic and other information were obtained from patient records using a structured pro forma. Retrieved data were entered into Microsoft Excel and exported to IBM Statistical Package for the Social Sciences version 21 for statistical analysis.
Data were tested for normality using Kolmogorov–Smirnov Statistics before the selection of statistical methods. Comparison between proportions employed Fisher’s exact test. P < 0.05 was considered statistically significant.
RESULTS
[Table 1] shows that the mean age of the study population was 47.86 years.
| Variables (n=78) | Frequency (n) | Percentage |
|---|---|---|
| Age in years | ||
| 16–25 | 0.00 | 0.00 |
| 26–35 | 14.0 | 18.0 |
| 36–45 | 28.0 | 35.9 |
| 46–55 | 22.0 | 28.2 |
| 56–65 | 11.0 | 14.2 |
| 66–75 | 3.00 | 3.80 |
| Mean age (SD): 47.86±10.84 | ||
| Age at menarche | ||
| 9–11 years | 9 | 11.5 |
| 12–14 years | 63 | 80.8 |
| 15–17 years | 6 | 7.7 |
| Parity | ||
| Para 0 | 7 | 9.0 |
| Para 1–4 | 50 | 64.1 |
| ≥Para 5 | 21 | 26.9 |
| Side affected | ||
| Left | 23 | 29.5 |
| Right | 24 | 30.8 |
| Both sides | 31 | 39.7 |
SD: Standard deviation
About 80% of patients reached menarche between 12 and 14 years, 64% had 1–4 children, and 26% had more than five children.
[Table 1] also outlines the laterality of breast cancer in the patients studied.
The most common findings on general clinical examination were anemia (43.6%), cachexia (39.7%), and hepatomegaly (11.5%).
On breast examination, the most common findings were axillary lymphadenopathy (87.2%), nipple changes (67.9%), peau d’orange (64.1%), skin nodules (64.1%), and chest fixity (60.3%).
This is a testament to the general late presentation in this cohort.
[Figure 3] shows that 29.5% of patients had evidence of pleural metastases, 19.2% had liver metastases, and 25.6% had spread to multiple sites.
[Table 2] shows that there was a statistically significant difference in the pattern of spread according to age, with the central nervous system and spinal spread being more common in younger patients.
| Spread | n | Mean Age±SD |
|---|---|---|
| Pleural effusion | ||
| Yes | 23 | 45.6±10.0 |
| No | 55 | 48.8±11.1 |
| t=1.16; P=0.249 | ||
| Liver spread | ||
| Yes | 15 | 45.6±10.0 |
| No | 63 | 48.8±11.1 |
| t=1.16; P=0.249 | ||
| Bone spread | ||
| Yes | 5 | 38.8±4.7 |
| No | 73 | 48.5±10.9 |
| t=1.97; P=0.053 | ||
| CNS spread | ||
| Yes | 5 | 39.0±6.8 |
| No | 73 | 48.6±10.8 |
| t=2.13; P=0.036* | ||
| Spine spread | ||
| Yes | 9 | 40.8±6.3 |
| No | 69 | 48.9±11.0 |
| t=2.26; P=0.026* |
[Table 3] shows that 22.8% of patients did not undergo abdominal ultrasound scans. This was due to either financial constraints or the scanning machine being out of service at the time of the request.
| Abdominal ultrasound findings | Number | % |
|---|---|---|
| Scan not done | 22 | 22.8 |
| Normal scan | 48 | 61.5 |
| Hepatomegaly/nodules | 05 | 6.40 |
| Pleural effusion | 03 | 3.84 |
| Total | 78 | 100 |
About 61.5% of patients had a normal abdominal scan, 6.5% had hepatomegaly or hepatic nodules, and 3.84% had evidence of pleural effusion.
Table 4 shows that sixty-nine patients (88.5%) had invasive ductal carcinoma as a histological diagnosis while 48 patients (61.0%) were premenopausal. Sixty-nine patients (88.5%) had invasive ductal carcinoma as a histological diagnosis while 48 patients (61.0%) were premenopausal.
| Variables | Premenopausal | Menopausal | Total |
|---|---|---|---|
| Ductal carcinoma in situ | 1 | 0 | 1 |
| Inflammatory breast carcinoma | 1 | 0 | 1 |
| Lobular carcinoma in situ | 1 | 0 | 1 |
| Mucinous carcinoma | 1 | 0 | 1 |
| Mixed invasive ductal and mucinous carcinoma | 1 | 0 | 1 |
| Invasive lobular carcinoma | 4 | 0 | 4 |
| Invasive ductal carcinoma | 39 | 30 | 69 |
| Total | 48 | 30 | 78 |
Figure 1 shows findings on general examination. 43.6% of patients had anaemia, 39.4% were cachexic,11.4% had developed hepatomegaly, 9.0% ascites while only 5.0% had jaundice.
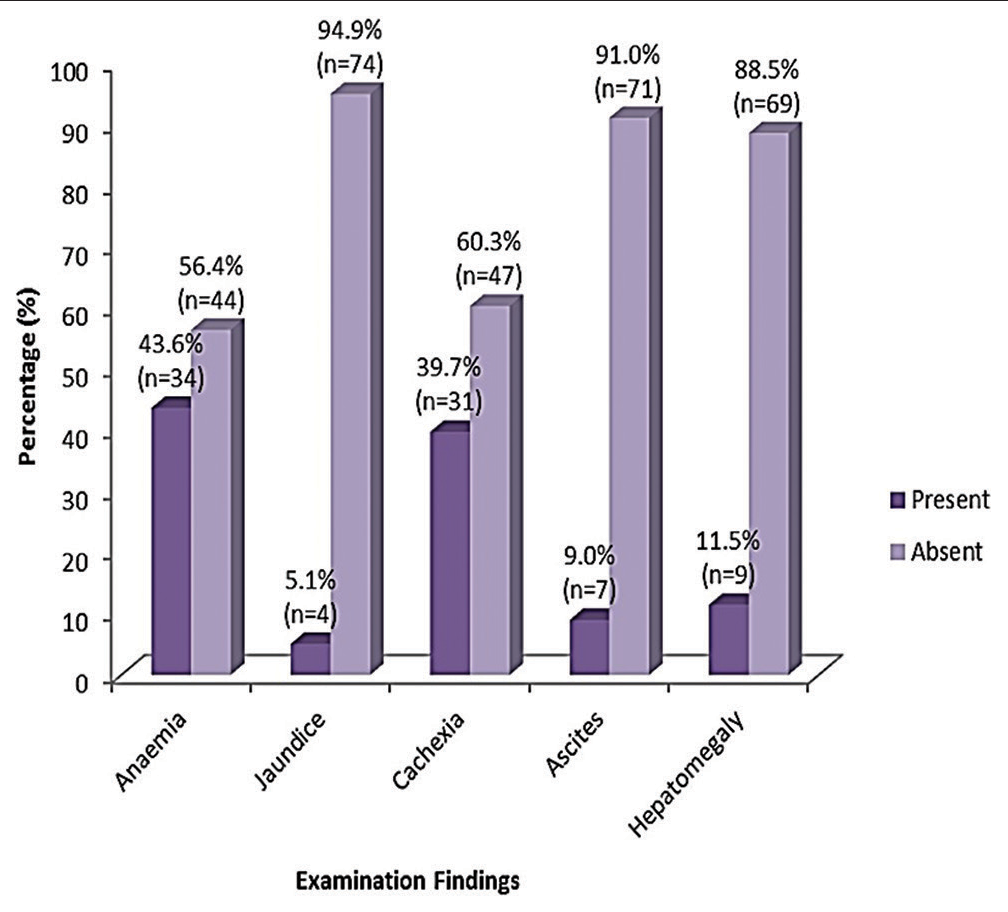
- Findings on general examination.
Figure 2 shows that on breast examination 87.2% of patients had already developed axillary lymphadenopathy. 67.9% had nipple changes and 64.1% of patients had peau d’orange and skin nodules.
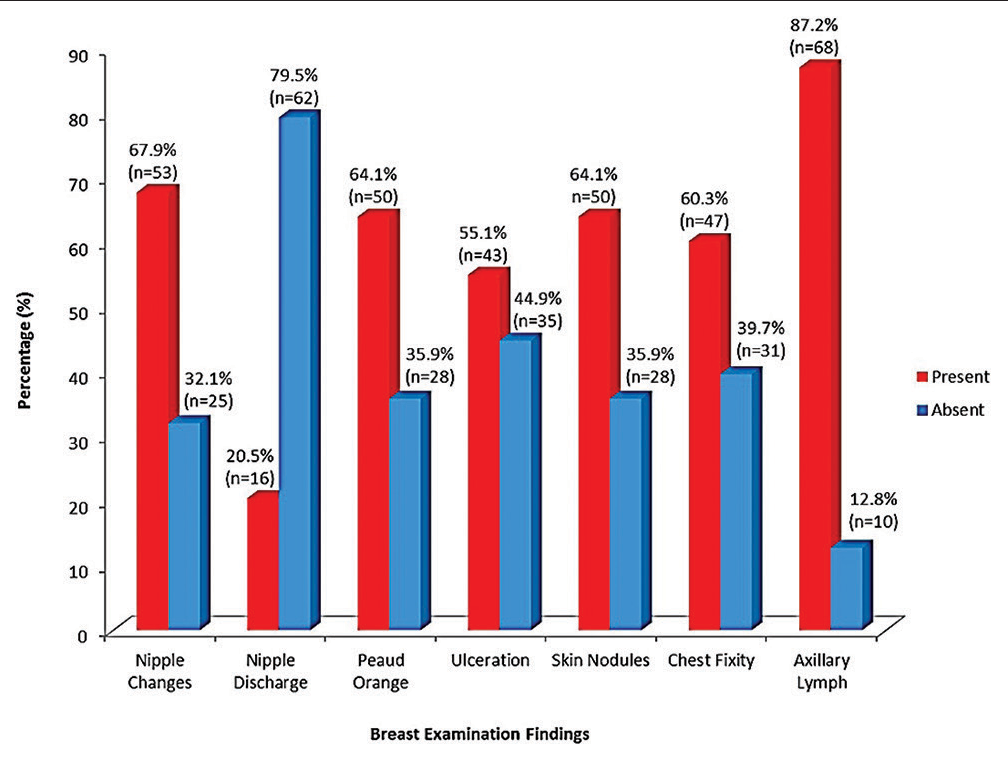
- Findings on breast examination.
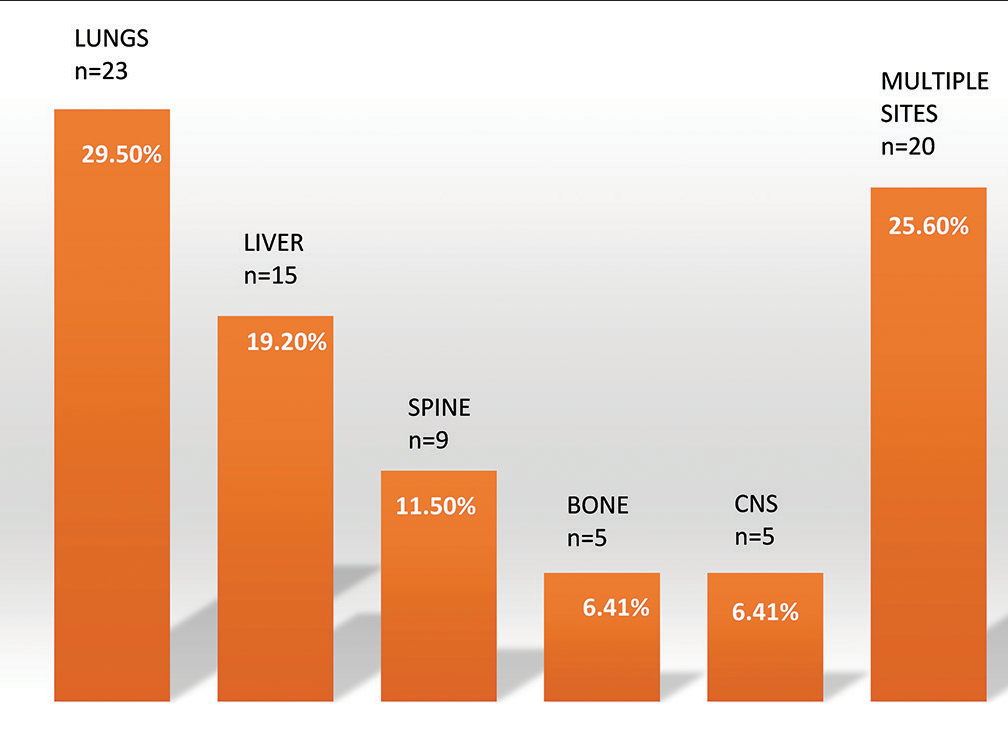
- Sites of metastasis.
60.3% had fixity to the anterior chest wall and 55.1% developed breast ulceration.
Only 20.5% of patients were found to have nipple discharge.
DISCUSSION
The mean age of the study population was 47.86 years with 53% falling into the childbearing age group. About 61% of the studied patients were premenopausal.
The most common findings on general clinical examination were anemia (43.6%), cachexia (39.7%), and hepatomegaly (11.6%). These are all pointers to the advanced stage at the initial presentation.
In addition, breast examination revealed axillary lymphadenopathy (87.2%), nipple changes (67.9%), peau d’orange (64.1%), skin nodules (64.1%), and chest fixity (60.3%).
There was no significant laterality in the breast cancer with 30.8% involving the right and 29.5% on the left. This differs from the findings of Mokone-Fatunla et al. in South Africa where left-sided breast cancer was more common.[8] The confounding factor in our study, however, was the fact that both breasts were involved in 39.7% of patients.
The most common sites of metastasis were the lungs (29.6%), liver (19.2%), and multiple sites (25.6%). This is different from the studies of Wu et al. which showed the bones to be the most common site, followed by lung, liver, and brain.[9-11]
Liver metastasis (19.2%) was higher than the 5.2% reported by Hoe et al. in Southampton.[12-14] It is important to note that 22.8% of patients were unable to carry out abdominal ultrasound scans due to financial constraints or challenges with the machine. There, thus, exists the possibility that liver metastases might be higher than reported.
Our study showed a statistically significant occurrence of spinal and central nervous system spread in patients younger than 48 years. This is in keeping with the findings of Tsukada et al.[15,16] and Warrior et al.[17]
The main implication of these findings is that a majority of our patients fall into the young, childbearing group and present late in the hospital. This has an adverse effect on outcome. Similar demographic and temporal presentations were found by Olayide et al. in Lagos,[18] Agbo et al.,[19] and Ezeome in Enugu.[20]
Limitations of the study include the fact that it is a retrospective study. The relatively small sample size is also a further limitation influenced by reduced hospital attendance in the immediate post-COVID period. A larger prospective study is planned in the future during which funding will be sought to enable more imaging and staging investigations to be done.
CONCLUSION
Late presentation remains the bane of cancer treatment in Nigeria. The situation is particularly dire in Yenagoa, Bayelsa State where non-hospital treatment is the norm. Eventual hospital presentation revealed that most of these patients had already developed metastases to the lungs liver and other organs. Most of these metastases resulted in mortalities. The concept of palliative care is not well developed in our center and many others in Nigeria.
Recommendations
Creation and development of awareness is key to urgently addressing these issues and will require a coalition of government and non-governmental agencies. Initiatives to promote awareness of breast and other cancers should emphasize the importance of early presentation in hospitals. Public enlightenment programs should emphasize the importance of breast self-examination and screening. Legislation may be required to criminalize the treatment of such cases outside a hospital setting.
Subsidized health-care programs will benefit patient access to investigations and treatment. While emphasis should be on prevention and early diagnosis, budgetary provision for the development of palliative care programs for cancer patients should be made.
Acknowledgments
We acknowledge the Tertiary Education Trust Fund which provided the funding for this study.
Ethical issues
The approval of the Research Ethics Committee of the Federal Medical Center Yenagoa was obtained.
Declaration of patient consent
Patient consent not required as patient’s identity is not disclosed or compromised.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The author(s) confirms that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Tertiary Education Trust Fund (TETFUND).
References
- The global burden of cancer: Priorities for prevention. Carcinogenesis. 2010;31:100-10.
- [CrossRef] [PubMed] [Google Scholar]
- Breast cancer in North Central Nigeria: Challenges to good management outcome. Int Surg J. 2019;6:3105-10.
- [CrossRef] [Google Scholar]
- Clinical course of breast cancer patients with liver metastases. J Clin Oncol. 1987;5:773-82.
- [CrossRef] [PubMed] [Google Scholar]
- Sabiston textbook of surgery: The biologic basis of modern surgical practice (19th ed). Netherlands: Elsevier; 2017. p. :1287-300.
- [Google Scholar]
- Organotropism: New insights into molecular mechanisms of breast cancer metastasis. NPJ Precis Oncol. 2018;2:4.
- [CrossRef] [PubMed] [Google Scholar]
- Molecular mechanisms of breast cancer metastasis and potential anti-metastatic compounds. Anticancer Res. 2018;38:2607-18.
- [CrossRef] [Google Scholar]
- Laterality of breast cancer at Dr George Mukhari academic hospital. S Afr J Surg. 2019;57:55-61.
- [CrossRef] [Google Scholar]
- The effect of distant metastases sites on survival in de novo stageIV breast cancer: A SEER database analysis. Tumour Biol. 2017;39:1010428317705082.
- [CrossRef] [PubMed] [Google Scholar]
- Liver metastases from breast cancer: The relationship between clinical, biochemical and pathological features and survival. Eur J Cancer Clin Oncol. 1990;26:574-7.
- [CrossRef] [PubMed] [Google Scholar]
- Clinical landscape of cancer metastases. Cancer Med. 2018;7:5534-42.
- [CrossRef] [PubMed] [Google Scholar]
- Breast liver metastases-Incidence, diagnosis, and outcome. J R Soc Med. 1991;84:714-6.
- [CrossRef] [PubMed] [Google Scholar]
- Prognostic factors for patients with hepatic metastases from breast cancer. Br J Cancer. 2003;89:284-90.
- [CrossRef] [PubMed] [Google Scholar]
- Bone metastasis pattern in initial metastatic breast cancer: A population-based study. Cancer Manag Res. 2018;10:287-95.
- [CrossRef] [PubMed] [Google Scholar]
- Central nervous system metastasis from breast carcinoma. Autopsy study. Cancer. 1983;52:2349-54.
- [CrossRef] [PubMed] [Google Scholar]
- Distinct organ-specific metastatic potential of individual breast cancer cells and primary Tumours. J Clin Invest. 2005;115:44-55.
- [CrossRef] [PubMed] [Google Scholar]
- Modern management and diagnostics in HER2+ breast cancer with CNS metastasis. Cancers (Basel). 2023;15:2908.
- [CrossRef] [PubMed] [Google Scholar]
- Level of awareness and knowledge of breast cancer in Nigeria. A systematic review. Ethiop J Health Sci. 2017;27:163-74.
- [CrossRef] [PubMed] [Google Scholar]
- Delays in presentation and treatment of breast cancer in Enugu, Nigeria. Niger J Clin Pract. 2010;13:311-6.
- [Google Scholar]




