
Translate this page into:
Anatomical features of the brain of patients with stroke (cerebrovascular accident) relative to types, sites, and shapes using computed tomography scan
*Corresponding author: Samson O. Paulinus, Department of Radiography and Radiological Science, University of Calabar, Calabar, Nigeria. samsonpaulinus@unicaledu.ng
-
Received: ,
Accepted: ,
How to cite this article: Udo-Affah GU, Paulinus SO, Eru EM, Igiri AO, Egbe NO. Anatomical features of the brain of patients with stroke (cerebrovascular accident) relative to types, sites, and shapes using computed tomography scan. Calabar J Health Sci 2020;4(2):79-83.
Abstract
Objectives:
Stroke is becoming a very common disease, giving rise to an increased morbidity and mortality globally; yet, its diagnosis is shrouded in the phrase “cerebrovascular accident.” The objectives of the study were to evaluate the various types, sites, and shapes of stroke presentation using computed tomography (CT) scan.
Material and Methods:
A total of 500 subjects indicative of stroke referred for cranial CT scans were recruited at the Jos University Teaching Hospital, Jos and the Asi-Ukpo Hospital, Calabar. With ethical approval, a proportionate random probability sampling method was used to obtain archived cranial CT images of the different types, sites, and shapes of the lesions, viewed directly from the CT scanners. Data obtained were analyzed using Statistical Package for the Social Science and results expressed as percentages and frequencies at P < 0.05.
Results:
The highest occurring type of stroke was ischemic (63.2%). Others were hemorrhagic (22.8%), cerebral atrophy (4.2%), cerebral infarct with atrophy (1.6%), intracerebral (0.8%), subarachnoid (1.4%), and subdural hemorrhage (0.8%). The left parietal lobe (24.8%) was the most common site of stroke occurrence while the left occipital, left temperoccipital, and left temperoparietal lobes had 7.6%, 7.4%, and 5.6%, respectively. Furthermore, 30.8% of cases presented as either oval hyperdense or hypodense lesions. Irregular lesions were 21.8% of cases while triangular, circular, and rectangular lesions occurred in 11.6%, 8.4%, and 6.4% of cases, respectively. Meanwhile, 8.0% of cases had normal CT brain scan that presented as stroke mimics on pattern recognition.
Conclusion:
The study revealed a distorted gross anatomy of the brain with preponderance of left-sided intracerebral ischemic stroke mostly in the left parietal lobe that presented as oval hyperdense and hypodense lesions in the sampled Nigerian population.
Keywords
Computed tomography scan
Ischemic
Shapes
Sites
Stroke

INTRODUCTION
Stroke or cerebrovascular accident occurs when there is cessation of blood flow to any part of the brain.[1] If the brain is subjected to hypoxic condition for longer than a few seconds, the brain cells deprived of oxygen will begin to die, causing permanent damage.[1,2] Two major types of strokes are identified; ischemic and hemorrhagic.[1,2] Ischemic stroke occurs when a clot blocks blood vessels that supply blood to the brain.[3] Clogged arteries, fat cholesterol, and other substances collected on the arterial wall form a sticky substance called plaque. This occurs either by an embolus becoming wedged in an artery supplying blood to the brain or the formation of blood clot in one of the cerebral arteries (thrombosis).[3,4] Ischemic stroke can also be caused by stenosis. This can occur in large or small arteries called large vessel disease (LVD) or small vessel disease (SVD), respectively. In SVD, a very small infarction sometimes called a lacunar infarction, results.[4] Whenever there is atherosclerosis (deposits of plaque build-up along the inner walls of large and medium sized arteries, causing thickening, hardening, and loss of elasticity of artery walls along with decreased blood flow), there must be stenosis. Atherosclerosis is the most common blood disease that causes stenosis.[4,5] Depending on the location of the blockage, ischemic stroke can affect sensation, speech, behavior, thoughts, memory, or emotions including one side of the body that may become paralyzed or weak. It has been reported that ischemic stroke occurs more commonly on the left hemisphere compared with the right hemisphere.[4,6] A hemorrhagic stroke occurs when blood vessel(s) in the brain burst or leak, causing blood to accumulate, compressing the surrounding brain tissues, and killing neurons.[1] It can also occur as a result of a bleeding aneurysm, an arterial wall breaks up, or a cerebral arteriovenous malformation.[1,7-9] The necessity to address the issue of stroke remains an invaluable contribution to human wellness, especially among the aged. It, therefore, becomes very imperative since its effects are not only limited on the aged but also among the younger people.[3] The negligence and uninterested approach in the management and treatment of stroke do not give patients better chances of survival, evidenced with scanty research that leaves people still very much uninformed. The diagnosis of stroke depends solely on the clinical assessment and imaging studies, for example, the conventional X-rays and the computed tomography (CT) scans. The CT scan examination is fast becoming a modality of choice for the management of severe stroke cases. However, the gap in the appreciation of CT anatomical features of stroke is still less understood, hence, the need to recognize effectively, the different pattern according to types, shapes, and sites presented in the study population for us to have good and accurate diagnosis taking cognizance of possible mimics of stroke.
MATERIAL AND METHODS
A total of 500 subjects, aged from <15 to >90 years, indicative of suspected stroke and referred for brain CT scan at the Jos University Teaching Hospital (JUTH), Jos and the Asi-Ukpo Hospital, Calabar, were recruited. With ethical clearance and approval (JUTH/DCS/ADM/127/XIX/6391), a proportionate random probability sampling method was used to obtain archived cranial CT images of the different types, sites, and shapes of the lesions noted in the sampled population. These images were viewed and recorded directly from the CT scanners; a bright speed 4-slice CT scanner in the CT suites of the Radiology Department, JUTH, Jos, and a 16-slice 385 CT scanner of the Asi-Ukpo Hospital, Calabar, over a period of 25 months. Patients with severe trauma, transient ischemic attack, and arteriovenous malformations including those with non-diagnostic image quality were excluded from the study. With the subjects in supine position, images used were observed using axial sections of the brain from the vertex of the skull to its base with the patient head placed on the headrest of the CT scanner and both arms by the sides. Observation showed that standard protocols were maintained in both hospitals. These include slice thickness 2.5 mm–5 mm, table increment 10 mm, 120 kVp, 300 mAs, standard algorithm, scan of view 25 cm, display of view 25 cm, window width of 150/100/80, and a window level 30. Parameters noted and recorded were the stroke types, sites, and shapes of the lesions in the substance of the brain. Data were analyzed using the Statistical Package for the Social Sciences and results expressed as percentages and frequencies at P < 0.05 taken to be the level of significance.
RESULTS
Results of the assessment of types of stroke are displayed in Table 1. It is evident that the most common type was ischemic (63.2%). Others were hemorrhagic (22.8%), cerebral atrophy (4.2%), cerebral infarct with atrophy (1.6%), intracerebral hemorrhage (0.8%), subarachnoid hemorrhage (1.4%), and subdural hemorrhage (0.8%). However, 5.2% of cases presented as stroke mimics.
| Stroke | Number of cases | Percentage |
|---|---|---|
| Ischemic | 316 | 63.2 |
| Hemorrhagic | 114 | 22.8 |
| Cerebral atrophy | 21 | 4.2 |
| Mimics | 26 | 5.2 |
| Cerebral infarct with atrophy | 8 | 1.6 |
| Intracerebral hemorrhage | 4 | 0.8 |
| Subarachnoid hemorrhage | 7 | 1.4 |
| Subdural hemorrhage | 4 | 0.8 |
| Total | 500 | 100 |
Chi cal.=3.751; df=8; P<0.05
The left parietal lobe (24.8%) was the most common site of stroke occurrence while the left occipital, left temperoccipital, and the left temperoparietal lobes had 7.6%, 7.4%, and 5.6% of cases, respectively. Other sites of stroke occurrence include the parietal (4.6%), right temperoparietal (3.6%), left frontal (2.4%), left temporal (2.8%), right frontal (2.4%), right temperoccipital (3.8%), temperoccipital (2.8%), occipital (2.0%), right occipital (2.6%), temporal (2.4%), frontal (1.8%), left parieto-occipital (2.4%), parieto-occipital (1.8%), right parieto-occipital (1.6%), intracerebral/right temperoparietal (1.6%), left temperoparieto-occipital (1.8%), temperoparietal (0.8%), and others (0.4%). These results are presented in Table 2.
| Location | No | % |
|---|---|---|
| Left parietal | 124 | 24.8 |
| Mimics | 65 | 13.0 |
| Left occipital | 38 | 7.6 |
| Left temperoccipital | 37 | 7.4 |
| Left temperoparietal | 28 | 5.6 |
| Parietal | 23 | 4.6 |
| Right temperoparietal | 18 | 3.6 |
| Left frontal | 12 | 2.4 |
| Left temporal | 14 | 2.8 |
| Right frontal | 12 | 2.4 |
| Right temperoccipital | 19 | 3.8 |
| Temperoccipital | 14 | 2.8 |
| Occipital | 10 | 2.0 |
| Right occipital | 13 | 2.6 |
| Temporal | 12 | 2.4 |
| Frontal | 9 | 1.8 |
| Left parieto-occipital | 12 | 2.4 |
| Parieto-occipital | 9 | 1.8 |
| Right parieto-occipital | 8 | 1.6 |
| Intracerebral/right | ||
| Temperoparietal | 8 | 1.6 |
| Left temperoparieto-occipital | 9 | 1.8 |
| Temperoparietal | 4 | 0.8 |
| Others | 2 | 0.4 |
| Total | 500 | 100 |
Chi cal.=213.103; df=18; P<0.05
The different shapes of the lesions [Table 3] revealed that majority (30.8%) cases presented as either oval hyperdense or hypodense. Irregular lesions were observed in 21.8% of cases while triangular, circular, and rectangular recorded 11.6%, 8.4%, and 6.4% of cases, respectively. In addition, diffused, bean, pear, multiple, horseshoe, convex, and bilateral were other shaped lesions with 3.2%, 2.8%, 0.8%, 2%, 0.8%, 1.4%, and 2.0% of cases, respectively. Meanwhile, 8.0% of cases had normal CT brain scan that presented as stroke mimics on pattern recognition.
| Shape | No | % |
|---|---|---|
| Oval | 154 | 30.8 |
| Irregular Triangle Circular |
109 58 42 |
21.8 11.6 8.4 |
| Rectangular Diffused |
32 16 |
6.4 3.2 |
| Bean shape Pear shape Multiple Horseshoe shape Convex |
14 4 10 4 7 |
2.8 0.8 2.0 0.8 1.4 |
| Bilateral | 10 | 2.0 |
| Mimics | 40 | 8.0 |
| Total | 500 | 100 |
Chi cal.=33.231; df=12; P<0.05
DISCUSSION
In this study, the most common type of stroke was ischemic (63.2%). Other types were hemorrhagic (22.8%), cerebral atrophy (4.6%), cerebral infarct with atrophy (1.6%), intracerebral hemorrhage (0.8%), subarachnoid hemorrhage (1.4%), and subdural hemorrhage (0.8%). However, 5.2% of cases diagnosed to have had apparently normal cranial CT scans were inferred to be stroke mimics. Our results support a similar study that reported 70.0% of cases of ischemic stroke.[5] In addition, result of the present study is in consonant with similar works which inferred that ischemic stroke occurred more commonly.[5,6,9-11]
The most common site of stroke occurrence in the present study was the left region of the brain [Figures 1-3]. In this case, the middle cerebral artery (largest of the cerebral arteries and the most common artery involved in stroke), which supplies blood to the lateral surface of each hemisphere, on the left side of the brain was mostly affected. This accounts for 24.8% of cases in the left parietal lobe. Other regions of the brain affected with stroke in the present study include the left occipital, left temperoccipital, and the left temperoparietal lobes with 7.6%, 7.4%, and 5.6% of cases, respectively. These results support a similar work that stroke usually occurs on the left side of the brain in the middle cerebral artery, resulting to damage of the left parietal lobe, left frontal lobe, and the left temporal lobe.[11] The affected individual is usually unaware of the contralateral (opposite) site, causing disruption of the person’s body schema and spatial orientation, affecting balance and safety awareness.[11] Sometimes, the affected individual often denies that anything was wrong.[6,11] Meanwhile, 13% of cases of the study population were diagnosed to have had normal CT brain scan but inferred to be stroke mimics on pattern recognition [Figure 3]. This may be attributed to clinical entities such as transient hypoglycemia that produces a stroke-like appearance with hemiplegia and aphasia, mass lesions, for example, subdural hematoma, cerebral abscess, primary central nervous system tumors, and the metastatic tumors are among clinical conditions that simulate stroke.[12] However, stroke mimics help to identify seizures and post-seizure events that present as common causes of stroke-like conditions.[11,12]

- Axial computed tomography scan of the brain obtained at the level of the clinoid process indicated by the arrow showing intracerebral hemorrhagic stroke in the left temporal lobe.

- Axial computed tomography scan of the brain obtained at the level of the clinoid process indicated by the arrow showing intracerebral ischemic stroke in the left temporal region.
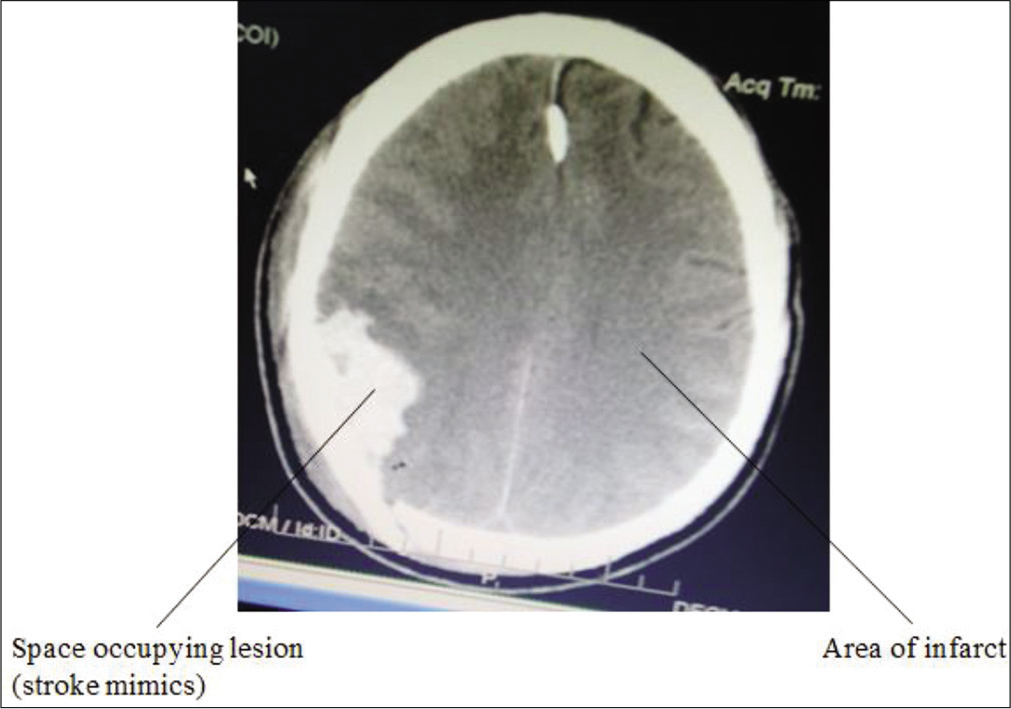
- Axial computed tomography scan of the brain obtained at the level of the clinoid process indicated by the arrow showing ischemic stroke characterized with space occupying lesion.
The different shapes of lesions with respect to the surrounding brain tissues were considered in the present study. Majority (30.8%) of the brains scanned, were characterized with either oval hyperdense or hypodense lesions. Irregular lesions were observed in 21.8% of cases while triangular, circular, and rectangular lesions had 11.6%, 8.4%, and 6.4% of cases, respectively. Others include diffuse shaped (3.2%), bean or kidney shaped (1.6%), pear shaped (0.8%), multiple shaped (2.0%), horseshoe shaped (0.8%), convex shaped (1.4%), and the bilateral shaped (2.0%), respectively. These findings reflect observations that the susceptibility of an individual to stroke is related to its size, shape, and location including the person’s age.[8]
The CT scan of the brain provides important clinical information as patient with either SVD or LVD detected after stroke occurrence is at greater risk of developing life-threatening conditions. This is because blood irritates delicate brain tissues and causes cerebral edema or tissue swelling including hematoma from the leaked blood vessel(s). This increases the mass effect, causing further damage and a general increase in intracranial pressure. In addition, brain cells beyond the rupture regions or sites are deprived of blood and are damaged.[1,7] This tangle of defective, thin-walled blood vessels and/or capillaries may bleed when subjected to pressure or damage, resulting to anatomical aberrations in the brain with greater risk of having or developing subsequent hemorrhagic or ischemic conversions. Therefore, the significance of sizes/ shape, sites, and location of lesions in the brain substance, measured by CT scan, cannot be overemphasized as this provides useful information to clinicians that may be helpful in prognosis.
CONCLUSION
The study revealed a distorted gross anatomy of the brain with preponderance of left-sided intracerebral ischemic stroke mostly in the left parietal lobe that presented as oval hyperdense and hypodense lesions. Meanwhile, there were no anatomical aberrations in some queried or perceived cases in the sampled Nigerian population, using cranial CT scans.
Acknowledgments
The authors acknowledged management of JUTH, Jos, and the Asi-Ukpo Hospital, Calabar, for the approval to use their facilities during the course of this study.
Declaration of patient consent
Patient’s consent not required as patients identity was not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Cohort study of effects of overweight and change in weight on risk of coronary heart disease in old age. Biomed J. 1997;314:1791-4.
- [CrossRef] [PubMed] [Google Scholar]
- Management of stroke rehabilitation: Veterans affairs/department of defense. J Rehabil Res Dev. 2010;47:1-43.
- [Google Scholar]
- Dual task effects of talking while walking on velocity and balance following stroke. Age Ageing. 2001;30:319-23.
- [CrossRef] [PubMed] [Google Scholar]
- Guidelines for the early management of patients with acute ischemic stroke: A guideline for healthcare professionals from the American heart association/American stroke association. Stroke. 2016;44:870-947.
- [CrossRef] [PubMed] [Google Scholar]
- Stroke admission in Kubua general hospital: A 30 month review. Sahel Med J. 2017;4:155-9.
- [CrossRef] [Google Scholar]
- Secondary prevention of atherothrombotic events after ischemic stroke. Mayo Clin Proc J. 2009;84:43-51.
- [CrossRef] [Google Scholar]
- Intracranial hemorrhage. Emerg Med Clin North Am. 2012;30:771-94.
- [CrossRef] [PubMed] [Google Scholar]
- CT and MRI early vessel signs reflect clot composition in acute stroke. Stroke. 2011;42:1237-43.
- [CrossRef] [PubMed] [Google Scholar]
- Heart disease and stroke statistics. A report from the American heart association. Circulation. 2011;123:208-9.
- [CrossRef] [PubMed] [Google Scholar]
- Predictors acute stroke mimics in 8187 patients referred to a stroke service. J Stroke Cerebrovasc Dis. 2013;22:397-403.
- [CrossRef] [PubMed] [Google Scholar]




