
Translate this page into:
Light-emitting diode bulb aspiration in a Nigerian child: A case report

-
Received: ,
Accepted: ,
How to cite this article: Adekanye AG, Francis PM, Eta JN, Lane ME. Light-emitting diode bulb aspiration in a Nigerian child: A case report. Calabar J Health Sci 2022;6:114-6.
Abstract
We report a 7-year-old girl who suddenly developed dyspnea, which was persistent, progressive, and severe with associated stridor and hoarseness following the aspiration of a light-emitting diode (LED) bulb that she held in her mouth while playing with her friend. Plain radiograph soft-tissue neck revealed a U-shaped radiopaque object in the glottis. An otolaryngologist extracted the LED bulb from the glottis through direct laryngoscopy under inhalational anesthetic agents without intubation. She was treated with analgesics and antibiotics and admitted into the ward for observation for 24 h, following which she was discharged home in satisfactory condition. Globally, there is a paucity of the literature on LED bulb aspiration, and the index case is the first documented in our center; hence, it is an addition to the body of the literature. Therefore, we strongly recommend that the differential diagnoses of a wire-like foreign body in the airway radiographs should include an LED bulb.
Keywords
LED bulb
Asphyxia
Child
Nigeria
Delayed diagnosis

INTRODUCTION
Foreign body (FB) aspiration is an otolaryngological emergency worldwide and the pediatric population suffers most from laryngeal and tracheobronchial FB aspiration. [1,2]
Etiologies of FB aspiration in children are multifactorial.[3] The types and nature of FB aspirated differ worldwide and range from ordinary organic to bizarre inorganic materials.[4] Recently, light-emitting diode (LED) bulbs have gained popularity in the toy industry due to their numerous physical advantages over older technologies. Studies on LED bulbs in the past focused principally on optical safety, with little concern about the risk of aspiration.[5] LED bulb aspiration is rare, and to the best of our knowledge, only a few cases are in the literature.[1,6]
However, because of the increasing use of LED bulbs as children toys accessories, medical health workers should be aware of the possibility of LED bulb aspiration.[1]
Health workers should be aware of the possibility of LED bulb aspiration.[1] We report a girl who held a led bulb in her mouth while playing with her friend but accidentally aspirated it.
Unfortunately, her mother’s first line of treatment includes digital maneuver and induction of vomiting, which were inappropriate techniques that should be discouraged.
CASE REPORT
A 7-year-old girl presented to the Children Emergency unit of the University of Calabar Teaching Hospital, Calabar, with 4-h history of sudden onset of progressive, persistent, and severe dyspnea, stridor, drooling of saliva, and hoarseness shortly after the insertion of the LED bulb in her mouth while playing in her house with one of her friends who brought three LED bulbs to her on a Sunday afternoon.
Immediately after the aspiration, she went to her mother to report the incident, and while talking with her, she reportedly fainted.
The mother attempted to remove the FB by digital maneuver and induction of vomiting, which proved abortive and reported to the children’s emergency ward of University of Calabar Teaching Hospital, Calabar for expert management.
On examination, the girl was in severe respiratory distress as evidenced by: A respiratory rate of 42 cycles/min, flaring alae nasi, accessory muscle of respiration in play as suprasternal, intercostal, and subcostal recessions, and inspiratory stridor, and SpO2 was 87%.
The oral and oropharyngeal examination revealed drooling of saliva, fair or dental hygiene, oral mucosa intact, the tongue was mobile in all directions, the tonsils and posterior pharyngeal walls were normal, and no bleeding or object was seen in the mouth.
Soft-tissue neck X-ray; anteroposterior and lateral views revealed a U-shaped radiopaque wire-like object in the glottis [Figure 1].
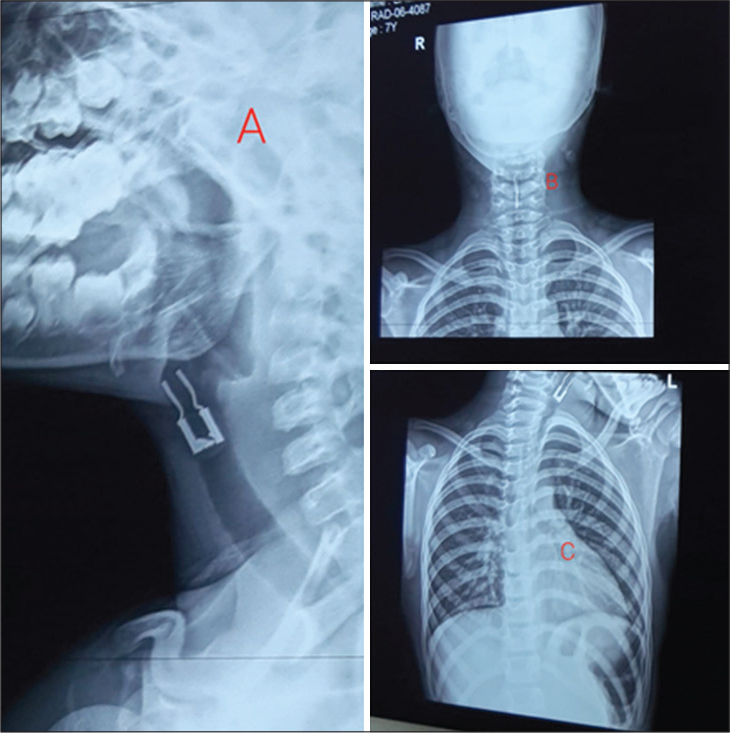
- The plain radiographies soft tissue neck of a 7-year-old girl who aspirated Led bulb. (a) showing an object: wire-like with two flanges and a base in the airway, at level of C3 to C5 vertebrae. (b) is anteroposterior view with the same foreign body in the airway of the same patient. (c) revealed normal radiograph of the chest, and the same foreign body in the larynx.
She was to have an emergency tracheostomy, followed by direct laryngoscopy and FB removal. While in the operative room, under an inhalational anesthetic agent, the anesthetist performed direct laryngoscopy, but the object was not visible in the supraglottic region. The child is still on a facemask, a quick look at the larynx with a rigid laryngoscope by an otolaryngologist revealed the FB wedged between the cords and removed with appropriate forceps [Figure 2]. Direct laryngoscopy was repeated, which yielded no other FB in the larynx. Likewise, there was no FB seen in the bronchi at the bronchoscopy. The operation was uneventful, and she was admitted for observation and placed on hydrocortisone and diclofenac suppository and discharged home after 24 h.
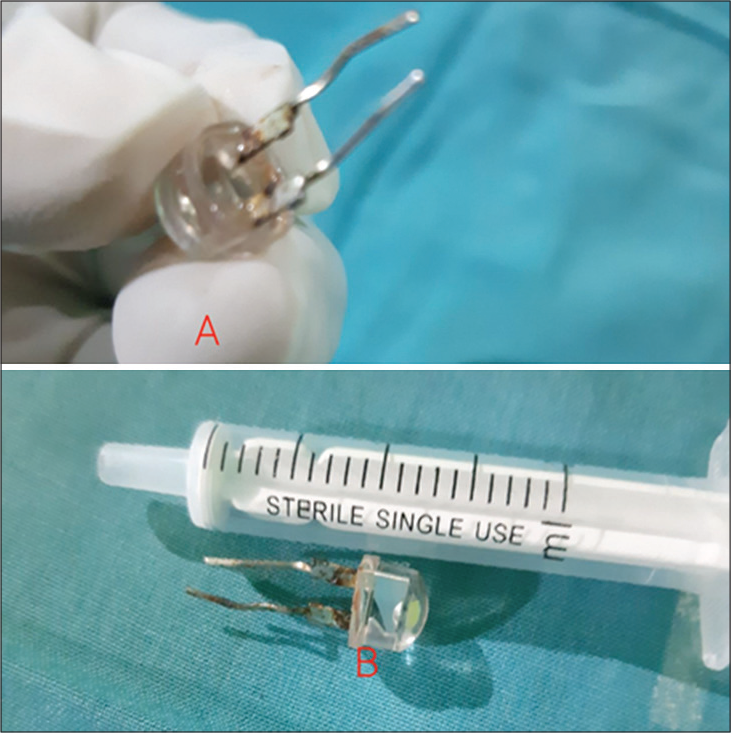
- A LED bulb removed (A) via direct laryngoscopy (B) from a 7 year old girl following accidental inhalation.
DISCUSSION
Children under age 5 are more susceptible to FB inhalation due to their oral tendency to play or run around with food pieces in the oral cavity, parental attitudes, lack of attention, and allowing small objects at the disposal of young children contribute to the high incidence of foreign bodies in children.[4,7] Our index case was a 7-year-old girl who carelessly kept an LED bulb in her mouth while playing with her friend.
Globally, FBA causes significant morbidity and mortality in children.[8] Inorganic foreign bodies when aspirated, portend grave danger with acute asphyxiation from total obstruction or respiratory difficulty from partial obstruction.[4] FBA clinical presentations varied from non-specific respiratory symptoms to respiratory failure with associated choking episodes; hence, its diagnosis could be delayed for weeks or even months, with increased complications and mortality. The delayed diagnosis could also arise from parental delay in seeking healthcare.[3] Furthermore, in the diagnosis of FBA, radiography is not a reliable method3 since many of these objects are radiolucent materials. However, radiography helps in confirming radiopaque foreign objects. The anatomical sites of the airway FB lodgment are the right main bronchus; the most common, due to its wide lumen and more vertical orientation,[6] followed by the left bronchus, trachea, subglottis, larynx, and carina.[4] The index case presented early to the hospital after aspiration with the pathognomonic symptoms of FBA. Although the plain radiograph soft-tissue neck revealed a wire-like FB in the larynx, it did not show the radiolucent part of the FB that was the main reason for airway obstruction at subglottic in our patient. Hence, the radiological features of this object were not complete.
The treatment options for FB aspiration include basic maneuvers such as forceful coughing, hardback slaps, abdominal thrust (Heimlich maneuver), and surgical interventions. The mother of our index patient did not offer any of these procedures to her child at home, but she induced vomiting with olive oil and attempted a digital maneuver to remove the FB. The two methods employed by the patient’s mother were not appropriate first-line techniques for the home management of FB aspiration. However, she took her daughter early to the hospital for an otolaryngologist’s intervention. Otolaryngologist promptly intervened and the FB was removed 6 h after the aspiration.
Continuous education of the caregivers and parents of children under 5 years on basic maneuvers implored for the extraction of FBA cannot be overemphasized. The parents and caregivers should avoid digital maneuver and vomiting induction on their children following FB aspiration. The American Academy of Pediatrics recommends education regarding aspiration/choking to all caregivers of children aged 6 months and above.[9]
Furthermore, immediate referral to otorhinolaryngologists as soon as FB aspiration is suspected because retrieval of aspirated FB is essential to prevent the risk of asphyxia, atelectasis or bronchiectasis, granulation tissue, recurrent pneumonia, and death.[10]
CONCLUSION
LED bulb aspiration is rare but should be a differential in children with FBA in our region. We advocate continuous education for parents and caregivers on basic maneuvers to remove aspirated foreign bodies. Furthermore, the caregivers/parents are encouraged to promptly consult the otorhinolaryngologist in all cases of suspected FB aspiration, and their early intervention is of the essence to prevent accompanied morbidity and mortality.
Acknowledgment
We acknowledge all the staff of the departments of anesthesia, otorhinolaryngology, pediatrics, and theater that participated in the treatment of this patient.
Declaration of patient consent
Patient’s consent not required as patients identity is not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Foreign body aspiration: Demographic trends and foreign bodies posing a risk. Indian J Otolaryngol Head Neck Surg. 2011;63:313-16.
- [CrossRef] [PubMed] [Google Scholar]
- Removal of inhaled foreign bodies-middle of the night or the next morning? Int Pediatr Otorhinolaryngol. 2009;73:1085-9.
- [CrossRef] [PubMed] [Google Scholar]
- Management of foreign bodies in the airway and oesophagus. Int J Pediatr Otolaryngol. 2012;76:S84-91.
- [CrossRef] [PubMed] [Google Scholar]
- Five centimeter concrete nail aspiration in a 2-year-old Nigerian child: A call for parental/care-givers' education. A case report. Case Rep Clin Med. 2015;4:261-5.
- [CrossRef] [Google Scholar]
- Safety assessment of near-infrared light-emitting diodes for diffuse optical measurements. Biomed Eng Online. 2004;3:9.
- [CrossRef] [PubMed] [Google Scholar]
- A Light bulb moment: An unusual cause of foreign body aspiration in children. BMJ Case Rep 2015
- [CrossRef] [PubMed] [Google Scholar]
- Pediatric nasal foreign bodies in Calabar: A review of 5-years experience. Niger J Med. 2020;29:20-3.
- [CrossRef] [Google Scholar]
- Foreign body inhalation in children: An update. Acta Otorhinolaryngol Ital. 2010;30:27-32.
- [Google Scholar]
- Prevention of choking among children. Pediatrics. 2010;125:601-7.
- [CrossRef] [PubMed] [Google Scholar]
- Pediatric airway foreign body retrieval: Surgical and anesthetic perspectives. Pediatric Anaesth. 2009;19:109-17.
- [CrossRef] [PubMed] [Google Scholar]




