
Translate this page into:
HIV serodiscordant and nondisclosure rates among married women living with HIV in a Southern Nigerian region

*Corresponding author: Ubong Bassey Akpan, Department of Obstetrics and Gynaecology, University of Calabar Teaching Hospital, University of Calabar, Calabar, Cross River, Nigeria. ubongabasiakpan@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Akpan UB, Arogundade K, Omoronyia E, Udo A, Ekott M, Etuk S. HIV serodiscordant and nondisclosure rates among married women living with HIV in a Southern Nigerian region. Calabar J Health Sci 2021;5:53-60.
Abstract
Objectives:
Intimate sexual partners’ disclosure of HIV positive status is vital in the control of HIV/AIDS pandemic globally. The disclosure rates vary from region to region. The aim of this study was to document the prevalence of HIV serodiscordance and partners disclosure rate; and also determine the associated factors among HIV positive married women living in Calabar region of Nigeria.
Material and Methods:
A cross-sectional survey was conducted among 260 married women, 18 years and above, receiving HIV care at various health institutions in the region. Data were analyzed using SPSS VERSION 23. Their demographic and health profile were presented in simple proportion and percentages while Chi-square test and logistic regression were used to determine the factors influencing patient’s HIV status disclosure with the level of significance set at 0.05.
Results:
A total of 254 compiled questionnaires were included in the analysis (response rate-97.7%). The serodiscordant rate was 50%. HIV status disclosure to partner was high, 89.4%. The main determinants of HIV status disclosure were good level of education (AOR = 2.2, 95% CI: = 1.75–2.53, P = 0.007) and long duration of ART use (AOR = 3.23, 95% CI = 2.78–4.15, P = 0.001) while women with high discordant rate were more likely to be divorced/separated (P = 0.012, OR = 1.67).
Conclusion:
Female education is an important factor in HIV control. Disclosure of HIV status is beneficial to the partner as it promotes safe sex practices and increases adherence to ART.
Keywords
HIV serodiscordance
HIV disclosure
Antiretroviral drugs
Female education
intimate partner’s violence

INTRODUCTION
Although HIV pandemic is a global problem, it is more predominant in sub-Sahara African countries.[1] Nigeria is the most populous country in Africa with an estimated population of 200 million people and is reported to be among the three countries with highest HIV prevalence in Africa.[2] Although there is a significant achievement in HIV control in the country as evidenced by the recent drop in the nations’ prevalence to 1.4%,[3] this huge population means that Nigeria still makes significant contribution to the global burden of HIV as an estimated 1.9 million people are living with HIV.[3]
The significant progress made in HIV/AIDS control is as a result of the increasing access to anti- retroviral drugs (ARDs) for people living with HIV/AIDs (PLWHA) such that between 2012 and 2013, there was a three-fold increase in people having access to ARDs and also the adoption of a test and treat policy since 2016 contributed greatly.[4]
Several measures have been considered to not only enhance uptake of HIV treatment among the infected but to prevent new infections in HIV seronegative sexual partners. The WHO reported 50% global serodiscordant rate of HIV among couples in a heterosexual union.[5] In a recent study in North America, about 40% of HIV positive pregnant women had a serodiscordant partner and 34% had a partner with an unknown HIV status.[6] A study has reported that disclosure of result occurs in 90% of women with serodiscordant partner and in 68% of women with partners whose HIV status was unknown.[6]
The WHO has enumerated many potential benefits to supporting couples to test together for HIV infection and to mutually disclose their HIV status.[5] This is important because together they can then make informed decisions about HIV prevention and other reproductive health issues.
Some of the potential benefits of Couples HIV Testing and Counseling (CHTC) according to WHO include: Increased uptake and adherence to prevention of mother to child transmission (PMTCT) which leads to decreased numbers of infants with HIV; HIV prevention within couples by the use of condoms and ARDs; increased marital cohesion that results in reduced intimate partners’ violence; and safer contraception/family planning methods with safer conception rates. Other benefits listed include prevention of HIV prevention in sexual partners by using condoms and ART; decreased stigmatization and normalization of infected partners and increased uptake and adherence to ART for one’s own health as well as decrease drug resistance, morbidity and mortality rates.[5] The WHO further emphasizes that couples and partners should be offered voluntary HIV testing and counseling with support for mutual disclosure.
However, partner’s disclosure rate in the developed countries like USA is as high as 90%[5] this may not be the case in the African region with high prevalence of HIV and coupled with cultural differences. Furthermore, the pattern of disclosure of HIV status varies among PLWHA from region to region.[7-9] While those in the developed countries may prefer disclosing HIV status to intimate sexual partners, women in some Asian and African countries may be more willing to disclose their status to close family members and friends.[7,8] These patterns are influenced by several factors including socio-economic profile, ethnic and cultural beliefs, gender-based practices, and indebt knowledge about the disease.[9-12] Hence, this study aimed to determine the disclosure rates and associated factors.
MATERIAL AND METHODS
Study setting, design, and population
The study was conducted in the old Calabar region of Southern Nigeria. It was the first Capital of Nigeria before the amalgamation of the southern and the northern protectorates during the colonial rule. This ancient city now has two administrative local government areas, namely, Calabar south and Calabar municipal councils. The population of Calabar is about 450,000.[13] It is the state capital of Cross River State of Nigeria. The prevalence of HIV infection in the state (Cross River State) is 1.7% from the recent National Demographic and Health Survey.[3] This was a cross-sectional survey using interviewer-administered questionnaire conducted among HIV positive married women. Multi-stage sampling was used to select participants. In the first stage, the health facilities were selected by simple random sampling. One tertiary, one secondary and six primary health facilities were selected. At the facility level, systemic sampling method was used to recruit respondents. HIV seropositive women who were receiving antiretroviral medication in these facilities were included in the study.
Sample size determination
The sample size for this study was calculated using Cochran formula for sample size determination.
n = Za2pq/d2
Where n = minimum sample size
Za = Standard deviate, a value at 95% confidence interval (CI) (= 1.96 t-test)
p = Prevalence of presence of the condition = 20% from a previous study
q= Probability of absence of the condition
d = Precision at 5%
Taking 15% HIV non-disclosure rates among intimate sexual partners, the sample size was thus calculated and made up to 260 to cater for no-response rate of 10%.
Instruments for data collection
The instrument for data collection for this survey was a semi-structured questionnaire. The questionnaire comprised six sections and 35 items. Section A elicited information on the socio-demographic characteristics of the participants. Section B obtained information on the health status of the participants, drugs/ART, previous obstetric history, HIV status of partners and infants, and disclosure of HIV status. Section C assessed various factors influencing result disclosure while Section D examined the level of knowledge on HIV/AIDS using a 7 point “Likert Scale Rating”[14] for level of knowledge modified to suite the purpose.
Validity and reliability of the instrument
To ensure the validity of the content of the instrument, the items in the questionnaire were given to public health experts for scrutiny, examination and comments. Thereafter, the total items as they were rated were computed to get the content validity index (CVI). A CVI score of point 0.73 was achieved. This was considered high enough for the study. Reliabilitrefers to the degree of consistency between two set of data or observation was obtained with the same instrument or equivalent forms of the instrument. For the purpose of this study, the test-retest method was used to ascertain the reliability of the instrument. Twenty copies of the questionnaire were administered to randomly selected HIV-positive women receiving ART at the Nigerian Military hospital in Calabar. These were those not included in the study population. Their identities were obtained, preserved, and kept confidential to aid re-administration of the questionnaire the 2nd time. After 2 weeks, similar copies of the questionnaires were again administered to same group of people and both sets were subjected to statistical analysis using Pearson’s Product Moment Correlation Coefficient Analysis. From the analysis, a reliability score of 0.78 was obtained indicating that the instrument is appropriate and suitable for use.
Sampling and data collection
A total of 260 respondents of 18 years and above participated in the study. In summary, the questionnaire retrieved information on bio-data, socio-economic profile, health condition, and HIV-related activities including where and when the diagnosis was made, commencement of ART, partners testing, results and disclosure, experiences regarding the medication and partners’ reaction as well as associated factors. They were encouraged to ask questions. They were allowed to express their thoughts on their experiences, motivations, and limitations.
Ethical issues
Participation was voluntary. Informed consent was obtained from each willing participant. Full confidentiality was assured. Approval was obtained from the Health Research Ethics Committee of the state ministry of health before commencement of the study (REG NO. CRSMOH/ HREC/2019/143).
Data management
Completed questionnaires were entered into SPSS spread sheet. Descriptive statistics were utilized to present data in frequencies, proportion and percentages. Bivariate and multivariate regression analyses were done to determine association between variables of interest. The level of significance was set at P ≤ 0.05.
RESULTS
Socio-demographic and health features
A total of 254 completed questionnaires were included in the analysis (97.7% response rate). Majority, 137 (53.9%) of them were 30 years and below. A significant proportion of them, 221 (87.0%) were in a stable monogamous relationship, 18 (7.1%) were in polygamous marriage while 15 (5.9%) were experiencing one form of marital disharmony or the other. Forty-one (16.1%) of the women were unemployed, and 87 (34.3%) had informal or vocational education [Table 1].
| Variables | Frequency (n=254) | Percentage |
|---|---|---|
| Age | ||
| 20-30 | 137 | 53.9 |
| 31-40 | 94 | 37.1 |
| 41-50 | 15 | 5.9 |
| 50 and above | 8 | 3.1 |
| Total | 254 | 100 |
| Current marital status | ||
| Monogamy | 221 | 87.0 |
| Polygamy | 18 | 7.1 |
| Divorced/Separated/Disharmony | 15 | 5.9 |
| Total | 254 | 100 |
| Number of children | ||
| 1-2 | 143 | 56.3 |
| 2-3 | 71 | 28.0 |
| 5 and above 6 | 11 | 4.3 |
| No child | 29 | 11.4 |
| Total | 254 | 100 |
| Estimated monthly income (US Dollars) | ||
| <#90,000 (200 dollars) | 100 | 39.4 |
| #90,000-#224,550 (200-499) | 105 | 41.3 |
| #225,000-#449,550 (499-999) | 32 | 12.6 |
| #450,000 and above (1000 and | 17 | 6.7 |
| above) | ||
| Total | 254 | 100 |
| Occupation | ||
| Unemployed | 41 | 16.1 |
| Artisan | 46 | 18.1 |
| Professional | 70 | 27.6 |
| Self employed | 77 | 30.3 |
| Schooling/Students | 20 | 7.9 |
| Total | 254 | 100 |
| Level of education | ||
| No formal education | 87 | 34.3 |
| Vocational education | 47 | 18.5 |
| Primary | 41 | 16.1 |
| Secondary | 42 | 16.5 |
| Tertiary | 37 | 14.6 |
| Total | 254 | 100 |
In assessing the level of income, only 49 (19.3%) earned up to 500 dollars per month. All of them had made at least one contact with a health facility or health personnel where maternal care and HIV testing and treatment were offered and only three (1.2%) of the respondents were yet to commence ART at the time of the survey while 38 (15%) of them had been on the ARV medication for 3 years and beyond. Apart from ART, many of them were on other chronic medications of which the most common was prophylactic antibiotics [Figure 1].
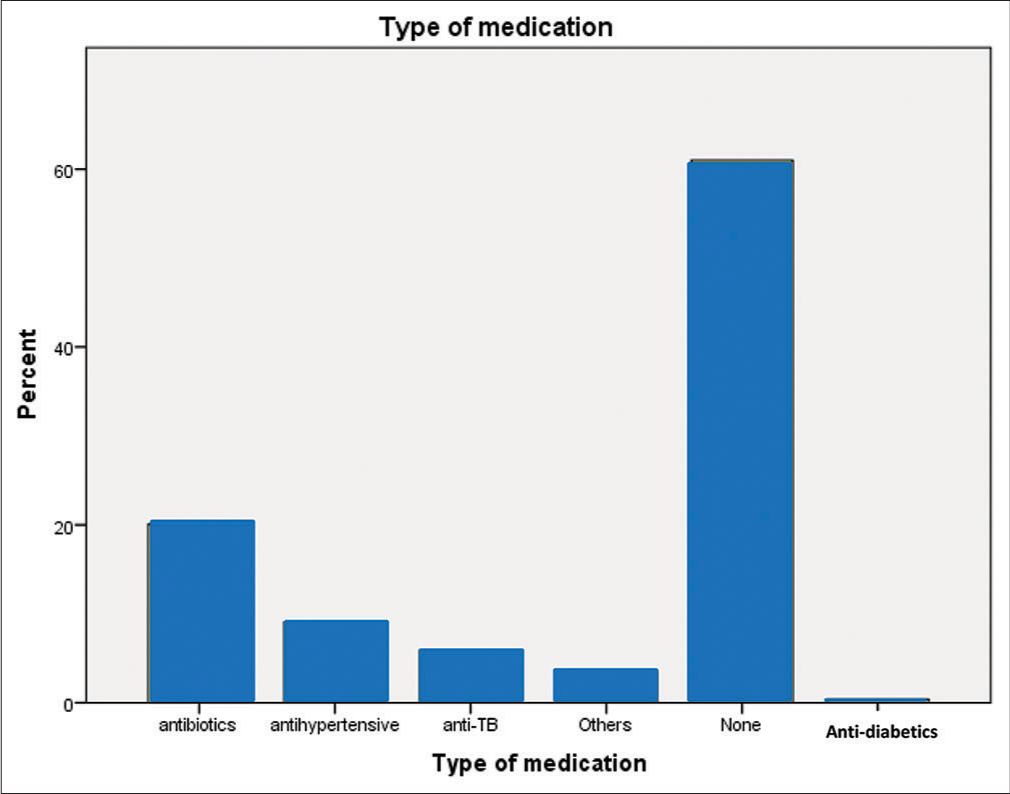
- Other medications apart from ART by respondents.
Serodiscordant prevalence and partners’ disclosure rate
The serodiscordant and the seroconcordant rates among the women whose partners’ HIV status were known to them were 127 (50.0%) and 100 (39.4 %), respectively, while 10.6% (27) of the respondents were yet to disclose their HIV status to their partners (Intimate partner disclosure rate of 89.4%) [Figure 2]. Eighteen (7.1%) of the 254 respondents reported nursing infants living with HIV.
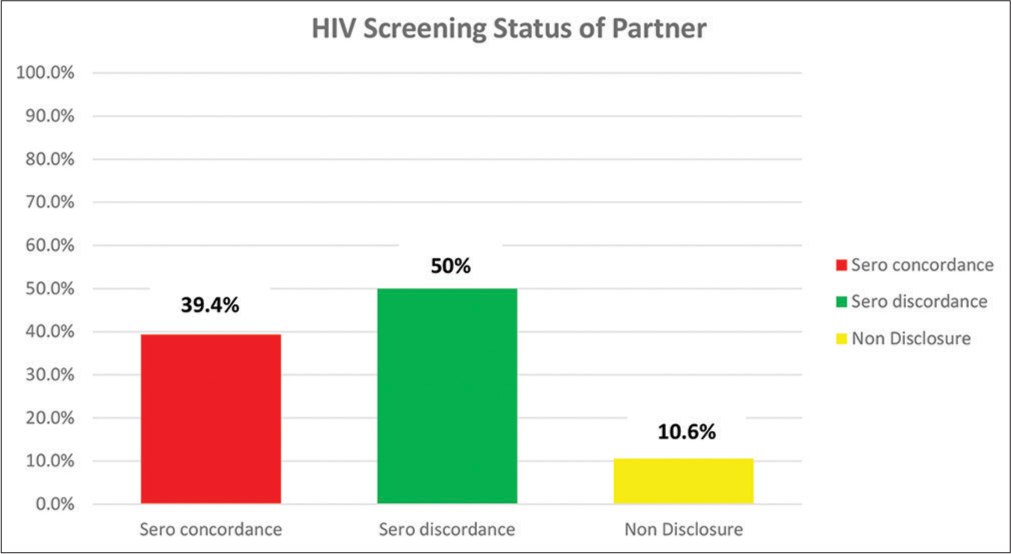
- HIV status of partners and non-disclosure of HIV status.
Among the 27 respondents who did not disclose their HIV status to their partners, 11 (40.7%) had confided in their close family relatives, 7 (25.9%) informed their close friends, and 4 (14.8%) had hinted their spiritual/religious leaders of their infection, while 5 (18.5%) were yet to disclose their HIV status to any person.
In assessing the pattern and medium through which HIV status was disclosed to partners, 173 (68.1%) informed their partner of their HIV status with the help of healthcare workers during counseling, and 106 (61.3%) of those who depended on health workers notified their partners during the period of ante natal care where they were diagnosed. Out of the remaining 54 (21%) respondents, 36 (14%) were able to notify their husbands by themselves while 18 (7%) involved friends, family relatives, and religious leaders as avenue for result disclosure.
Determinants of serodiscordance and non-disclosure of HIV status to partners
In determining the factors influencing HIV serodiscordant, the study revealed that women who had no education or vocational education were more likely to have partners with serodiscordant HIV results compared to women with formal education (Adjusted Odd Ratio [AOR] = 2.2, 95% CI = 1.75–2.53, P = 0.007). Women who were divorced or separated from their husbands reported 80% serodiscordant rate compared to the other women (48%); P = 0.012, AOR = I.67. Occupation/employment status, nature of living apartment and level of household income did not predict serodiscordant union. Table 2 summarizes how HIV result disclosure improves with the level of education attainment.
| Variables | HIV screening result of Partner | Total | ||
|---|---|---|---|---|
| Positive | Negative | Non-disclosure | ||
| Duration of ART | ||||
| <1 year | 44 | 47 | 21 | 112 |
| 1-2 year | 39 | 58 | 4 | 101 |
| 3 and above | 17 | 20 | 1 | 38 |
| Not on ART | 0 | 2 | 1 | 3 |
| Total | 100 | 127 | 27 | 254 |
| Marital status | ||||
| Polygamy | 12 | 5 | 1 | 18 |
| Monogamy | 87 | 110 | 24 | 221 |
| Divorced/separated/Disharmony | 1 | 12 | 2 | 15 |
| Total | 100 | 127 | 27 | 254 |
| Estimate of monthly family income | ||||
| <200 Dollas | 45 | 40 | 15 | 100 |
| 200-499 Dollas | 41 | 55 | 9 | 105 |
| 500-999 | 9 | 21 | 2 | 32 |
| 1000 and above | 5 | 11 | 1 | 17 |
| Total | 100 | 127 | 27 | 254 |
| Number of children | ||||
| 1-2 | 52 | 74 | 17 | 143 |
| 3-4 | 25 | 40 | 6 | 71 |
| 5 and above | 5 | 6 | 0 | 11 |
| 4=No child | 18 | 7 | 4 | 29 |
| Total | 100 | 127 | 27 | 254 |
| Level of education | ||||
| No vocational education | 21 | 56 | 10 | 87 |
| Vocational education | 19 | 20 | 8 | 47 |
| Primary | 20 | 17 | 4 | 41 |
| Secondary | 24 | 14 | 4 | 42 |
| Tertiary | 16 | 20 | 1 | 37 |
| Total | 100 | 127 | 27 | 254 |
| Occupation | ||||
| House wife | 22 | 16 | 3 | 41 |
| Artisan | 10 | 34 | 2 | 46 |
| Professional | 30 | 33 | 7 | 70 |
| Self employed | 31 | 36 | 10 | 77 |
| Student | 7 | 8 | 5 | 20 |
| Total | 100 | 127 | 27 | 254 |
| Nature of apartment | ||||
| Single apartment | 28 | 23 | 7 | 58 |
| Self-contained | 28 | 65 | 9 | 102 |
| Flat | 42 | 38 | 9 | 89 |
| Duplex | 2 | 1 | 2 | 5 |
| Total | 100 | 127 | 27 | 254 |
| Baby’s status | ||||
| Positive | 6 | 11 | 1 | 18 |
| Negative | 94 | 116 | 26 | 236 |
| Total | 100 | 127 | 27 | 254 |
| Maternal age | ||||
| 18-30 | 46 | 76 | 15 | 137 |
| 31-40 | 42 | 41 | 11 | 94 |
| 41-50 | 8 | 7 | 0 | 15 |
| 51 and above | 4 | 3 | 1 | 8 |
| Total | 100 | 127 | 27 | 254 |
ART: Antiretroviral therapy
Furthermore, in assessing the determinants of HIV non-disclosure to partners, women who were receiving ART for at least 1 year were more likely to disclose their HIV status to their husbands compared to women who were newly enrolled on treatment (P = 0.04) as shown in Table 3. Their knowledge on HIV treatment and prevention was rated as good, average or poor using standardized score scale. Overall, a good proportion 156 (61.4%) of the respondents exhibited good knowledge while only 17 (6.7%) had poor knowledge. However, this indebt knowledge on HIV did not significantly influence disclosure of HIV status to partners (P = 0.73). Similarly, increasing maternal age did not significantly correlate positively with disclosure of HIV status (Spearman’s correlation coefficient = −122, P = 0.053). Nursing an HIV positive infant and parity did not predict partners’ disclosure (P = 0.57; AOR = 0.56 and P = 0.086; AOR = 0.069), respectively.
| Variables | P value | Odd ratio (AOR) | 95% confidence interval |
|---|---|---|---|
| Antiretroviral therapy >1 year | 0.004* | 3.23 | 2.78–4.15 |
| Nursing HIV positive infants | 0.39 | 0.97 | 0.92–1.89 |
| Multiparity (>2 children) | 0.59 | 1.13 | 0.686–1.83 |
| Maternal disharmony (divorced/separated) | 0.0012* | 1.67 | 1.48–2.82 |
| Income status >200USD | 0.57 | 0.132 | 0.11–0.45 |
| Employment status | 0.97 | 0.134 | 0.10–1.20 |
| Nature of house (flat/ duplexes) | 0.989 | 1.24 | 1.08–1.44 |
| Formal education | 0.007* | 2.21 | 1.75–2.53 |
DISCUSSION
The study revealed a huge HIV burden among young women as majority of the respondents, 53.9% were below 30 years of age. Similar finding was reported in a South African study with 58% of the HIV-positive women being between the ages of 18–29 years.[15] This is in contrast to a recent published figure in the USA which suggested 5 times more new infections in young males than females.[16] This emphasizes the need to adopt different strategies depending on the regional demography in tackling the menace of HIV. For instance, a program that focuses on young male homosexuals may be effective in the developed countries, while a more holistic approach may be needed to reach young African women in heterosexual relationship.
The 50% HIV serodiscordant rate in this study is in line with the WHO global estimate of 20–60%.[5] Poverty, low status of women and negative gender based practices has been blamed for this disparity in HIV seroconversion among intimate couples.[17-20] Furthermore, in 2017, UNAIDS reported that up to a third of women living with HIV/AIDS (WLWH) in African region experienced gender based violence.[21] The 89.4% intimate partners’ HIV disclosure rate (10.6% non-disclosure) in this study was similar to 90% from developed countries[5] and 87% in Kenya[22] but comparably higher than the rates reported in other African countries.[9,23,24]
The high disclosure rate in this study could have been influenced by the health education and counseling received by the participants as all of them were recruited through various health facilities offering HIV care unlike in other community-based surveys. Furthermore, a significant proportion of them knew about their status during antenatal care where many of their spouses were also tested. Thus, active counseling by the trained health workers must have contributed to this positive change. The intimate partners’ disclosure and testing are cardinal factors in HIV control. The benefits include safe sex practices, increased adherence to ART, and PMTCT.[25] In addition, pre-exposure prophylaxis (PrEP) may be considered for the uninfected partner.[26] A recent study has shown that PrEP significantly reduced incidence of HIV infections among female commercial sex workers.[27]
Female education still remains one of the ways of promoting equality and empowerment for women to take reproductive and health sexual decisions. This is supported by the findings in this study about the influence of female education on partners’ disclosure of HIV status. Women who obtained formal education were significantly more likely to disclose their HIV status to intimate partners compared to women with informal or no education (Odd Ratio [OR] = 2.21, 95% CI = 1.78–2.67, P = 0.007). Similar findings have been reported.[28-30] Some of the reasons proffered for non-disclosure of HIV status to male spouses among infected women include potential risk of suffering gender-based violence such as emotional and verbal abuse by partner and family members, loss of financial support, and sex deprivation. Female education should, therefore, have a social stabilizing effect on families and societies. Educated women are better informed of the benefit of result disclosure in the control of a pandemic like HIV and are less likely to suffer social injustice.
About 6% of the respondents were either separated or divorced from their husbands. These women with marital disharmony reported higher rate of male partner serodiscordant rate (80%) compared to the women is stable relationship (50%), OR-1.6; P = 0.003. Discovery of partners’ HIV status could have played a role as the seronegative partners might have nursed the fear of being infected. This has been cited as a common factor in sex deprivation suffered by WLWH.[31] A previous study has showed that married women were 2.4 times more likely to transmit HIV to their sexual partners after 1 year of heterosexual relationship compared to divorced/widowed women.[32]
As shown in Table 3, whereas, high parity and nursing an HIV positive infant did not predict having a seropositive partner (P = 0.086, P = 0.569, respectively), the duration of ARV therapy by the women was positively associated with HIV negative status of the male partners. Women who were on the ART medication for at least 1 year were more likely to have serodiscordant spouses compared to those who initiated the medication <1 year (P = 0.004). Prolonged use of ART would decrease the viral load and the risk of HIV transmission to the uninfected partner. This has become a major intervention in the global control of HIV/AIDS.[31-33]
Maternal age did not significantly influence HIV status disclosure or being married to HIV negative partner: Younger maternal age (44%) versus older women, >30 years, (56%); (OR = 0.8, CI = 0.67–1.10). Findings from a previous study had suggested that young women being married to older male partners was associated with high HIV serodiscordance rates among couples.[14] Occupation is one of the socio-economic factors that can influence the disclosure of HIV status (OR = 0.134, 95% CI = 0.10–1.20). However, our study did not show any significant difference in the disclosure rates between the unemployed and the employed participants contrary to a previous report which suggested that good economic status promote HIV status disclosure.[18]
The study revealed that nature of apartment may not affect partner HIV status disclosure. Respondents who lived in multi-room apartments (flats or duplexes) did not show significant difference in concealing their HIV status from their spouses compared to the women that reside in single room apartments (P = 989, OR = 1.24, 95% CI = 1.08– 1.44). The ability to conceal vital health information from close family relatives may be influenced by the type of living apartment. For instance, being able to keep the drug container away from spouse may be difficult if the couple is living in a single room apartment compared to those who live in flats or duplexes. A study in Tanzania suggested that couples living far away from HIV counseling and testing centers were more likely to be serodiscordant compared to those who lived nearby.31
Our study focused on intimate partners’ disclosure. The previous studies have shown that WLWH may exhibit different preferences on who to disclose their status to including sexual partners, family members, friends, and colleagues.[12,13] However, our study revealed that among the women who did not disclose their status to their intimate partner, some have disclosed to family members, close friends, and religious leaders and only a minute number kept it to themselves. The need for emotional, psychological, and religious support may warrant this pattern of disclosure. It is also evidenced that most also utilized the help of healthcare workers to inform their partners after counseling.
Finally, majority of the respondents (61.4%), irrespective of their academic attainment, exhibited good knowledge about HIV transmission, treatment, and prevention. However, contrary to a previous report,[9] this in-depth knowledge did not significantly predict result disclosure to partners showing that social and cultural factors overshadowed it.
CONCLUSION
The serodiscordant rate in this study is in keeping with the global average. The HIV status disclosure is also encouraging.
To reduce the risk of HIV infection in the uninfected partners, there is need to encourage continuous education of the couples on ART and safe sex. It is recommended that the couples should be encouraged to utilize HIV counseling and testing together and mutually disclose their results to one another. Early diagnosis and commencement of ART by the infected partner as well as lifestyle modification are beneficial to couples.
Acknowledgments
The authors wish to acknowledge the staff of PEPFER clinic of the UCTH and other health facilities where the recruitment of participants was carried out.
Ethical approval
Approval was obtained from the Cross River State Ministry of Health Research Ethics Committee before commencement of the work.
Data availability
The data used to support the findings of this study are available from the corresponding author on request.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Ending AIDS Progress towards the 90-9090 Targets. Global AIDS Update, UNAIDS/JC2900E.
- [Google Scholar]
- Demographic dynamics and development in Nigeria. Afr Popul Stud. 2014;27:239-48.
- [CrossRef] [Google Scholar]
- Nigeria National HIV Prevalence Drops to 1.4 Percent. 2020. Available from: https://www.ghanahealthnest.com [Last accessed on 2020 Jan 14]
- [Google Scholar]
- Than Once Thought and Highlights Key Caps Towards Pro-Acting HIV Epidemic Control. 2019. Available from: https://www.cdc.gov [Last accessed on 2019 Dec 15]
- [Google Scholar]
- WHO: Couples HIV Testing and Counseling Including Antiretroviral Therapy for Treatment and Prevention in Serodiscordant Couples In: Recommendation for a Public Health Approach. Geneva, Switzerland: World Health Organization; 2012.
- [Google Scholar]
- Demographic and Health Survey (DHS) 2000-2010. 2010. Available from: http://www.measuredhs.com/surveys/dhs/start.cfm [Last accessed on 2019 Nov 03]
- [Google Scholar]
- Disclosure of HIV serostatus to sex partners in rural Louisiana. AIDS Care. 2006;18:S62-9.
- [CrossRef] [PubMed] [Google Scholar]
- Disclosure of HIV serostatus to sex partners: A new approach to measurement. Sex Transm Dis. 2006;33:102-5.
- [CrossRef] [PubMed] [Google Scholar]
- Factors affecting intention to disclosure HIV status among adult population in Sarawak, Malaysia. J Environ Public Health. 2018;2018:2194791.
- [CrossRef] [PubMed] [Google Scholar]
- Disclosure of HIV status: The role of ethnicity among people living with HIV in London. J Acquir Immune Defic Syndr. 2008;47:514-21.
- [CrossRef] [PubMed] [Google Scholar]
- Factors influencing social self-disclosure among adolescent living with HIV in Eastern Africa. AIDS Care. 2015;27:36-46.
- [CrossRef] [PubMed] [Google Scholar]
- Disclosure among people living with HIV/AIDS. Indian J Community Med. 2007;32:P280.
- [CrossRef] [Google Scholar]
- The effect of population explosion on family standard of living in Calabar, Nigeria. Eur Soc J. 2014;10:e1857-7431.
- [Google Scholar]
- Statistical Scale for Assessment of Knowledge and Attitude. 1932. Available from: https://www.geopoll.com [Last accessed on 2019 Oct 22]
- [Google Scholar]
- Determinants of disclosure and non-disclosure of HIV positive status by pregnant women in rural South Africa. SAHARA J. 2018;15:155-63.
- [CrossRef] [PubMed] [Google Scholar]
- Diagnosis of HIV infection in the United States and Dependent Areas, 2018. HIV Surveillance Report. 2020;31
- [Google Scholar]
- Gender perspective of risk factors associated with disclosure of HIV status, a cross-sectional study in Soweto, South Africa. PLoS One. 2014;9:e95440.
- [CrossRef] [PubMed] [Google Scholar]
- Facilitating HIV disclosure across diverse settings: A review. Am J Public Health. 2011;101:1011-23.
- [CrossRef] [PubMed] [Google Scholar]
- HIV/AIDS knowledge, self-efficacy for limiting sexual risk behavior and parental monitoring. J Pediatr Nurs. 2016;31:e63-9.
- [CrossRef] [PubMed] [Google Scholar]
- Intimate partner violence among HIV-serodiscordant couples in Durban, South Africa. S. Afr Med J. 2018;108:960-4.
- [CrossRef] [PubMed] [Google Scholar]
- UNAIDS HIV/AID Information. 2018. Available from: https://www.unaids.org [Last accessed on 2020 Apr 06]
- [Google Scholar]
- Prevalence and correlates of non-disclosure of maternal HIV status to male partners: A national survey in Kenya. BMC Public Health. 2018;18:671.
- [CrossRef] [PubMed] [Google Scholar]
- When do HIV-infected women disclose their HIV status to their male partner and why? A study in a PMTCT programme. Abidjan. PLoS Med. 2007;4:e342.
- [CrossRef] [PubMed] [Google Scholar]
- Social context of disclosing HIV test results in Tanzania. Cult Health Sex. 2012;14:53-66.
- [CrossRef] [PubMed] [Google Scholar]
- HIV-seroconversion among HIV-1 serodiscordant married couples in Tanzania: A cohort study. BMC Infect Dis. 2019;19:518.
- [CrossRef] [PubMed] [Google Scholar]
- Integrating oral PrEP delivery among african women in a large HIV endpoint-driven clinical trial. J Int AIDS Soc. 2020;23:e25491.
- [CrossRef] [PubMed] [Google Scholar]
- "I am still negative": Female sex workers' Perspectives on uptake and use of daily pre-exposure prophylaxis for HIV prevention in South Africa. PLoS One. 2019;14:e0212271.
- [CrossRef] [PubMed] [Google Scholar]
- Factors affecting HIV disclosure among partners in Morongo, Tanzania. Int J Afr Sci. 2019;10:49-54.
- [CrossRef] [Google Scholar]
- HIV-1 transmission within marriage in rural Uganda: A longitudinal study. PLoS One. 2013;8:1-8.
- [CrossRef] [PubMed] [Google Scholar]
- HIV/AIDS epidemic in India: Risk factors, risk behaviour and strategies for prevention and control. Indian J Med Res. 2005;121:356-68.
- [Google Scholar]
- Prevalence and predictors of HIV serodiscordance among cohabiting couples tested in Northern Tanzania. Pan Afr Med J. 2015;22:275.
- [CrossRef] [PubMed] [Google Scholar]
- Population HIV transmission risk for serodiscordant couples in Guangxi, Southern China: A cohort study. Medicine (Baltimore). 2018;97:e12077.
- [CrossRef] [PubMed] [Google Scholar]
- Awareness and factors that influence birth preparedness and complication readiness among pregnant women attending antenatal clinic in the General Hospital Calabar, Nigeria. Public Health Res. 2017;7:78-84.
- [Google Scholar]




