
Translate this page into:
Anesthesia equipment and their chain of survival

*Corresponding author: Queeneth Kalu, Department of Anaesthesiology, University of Calabar and University of Calabar Teaching Hospital, Eastern Highway, Calabar 5400, Cross River, Nigeria. queenidine@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Kalu Q, Edentekhe TA, Eguma S. Anesthesia equipment and their chain of survival. Calabar J Health Sci 2020;4(1):13-9.
Abstract
Objectives:
Anesthesia is a technology driven specialty, technological advancement in anesthesia and monitoring equipment has made sophisticated surgery possible. Safe anesthesia is possible when machines are in good condition. The chain of survival as used by the International Liaison Committee on Resuscitation refers to a series of actions that, properly executed, reduce the mortality associated with cardiac arrest. A similar chain can be applicable to anesthetic equipment for optimal patient care. Early acquisition of appropriate equipment, appropriate training of end users, prompt preventive maintenance, timely repair, and replacement at the end of the equipment lifespan. In 2002, the Federal Government of Nigeria (FGN) commissioned a project to refurbish eight teaching hospitals which was later upgraded to 14. This paper assessed the functional status of 10 frequently used equipment in anesthesia and intensive care units among the beneficiaries.
Material and Methods:
A structured questionnaire was sent to heads of anesthesia departments in the 14 beneficiary hospitals of the FGN/VAMED intervention. They reported on the status of 10 equipment commonly used by anesthetists in the operating rooms and intensive care units.
Results:
All hospitals had the equipment installed in the past 7–14 years with end user training on all the equipment, biomedical engineers were available in the immediate post-installation period. There has been no routine scheduled preventive maintenance of the equipment. Faulty equipment are being used in all the hospitals, 54.6% of the installed equipment are spoilt and no longer in use. The weakest link in the equipment chain of survival is the absence of preventive maintenance.
Conclusion:
Routine scheduled preventive maintenance and the constant availability of trained and skillful biomedical engineers will no doubt increase the lifespan of anesthetic equipment.
Keywords
Anesthesia
Equipment
Maintenance
Biomedical engineers
End user training

INTRODUCTION
Technological advancement in anesthesia, and the use of monitoring equipment, has made sophisticated surgeries possible. Anesthesia equipment can be technically complex and require expertise to use, maintain, and repair. Medical equipment generally have an expected lifespan of about 10 years[1] depending on the type of equipment, frequency of use, and maintenance. Safe anesthesia is enhanced when equipment are in good condition. When equipment are faulty or unavailable, patients may suffer significant risks and service delivery may be hampered. The chain of survival as used by the International Liaison Committee on Resuscitation refers to a series of actions that, properly executed, reduce the mortality associated with cardiac arrest.[2] A similar chain can be applicable to anesthetic equipment for optimal patient care. Acquisition of appropriate equipment, training of end users, prompt preventive maintenance, timely repair, and replacement constitute components of this chain. In 2002, the Federal Government of Nigeria (FGN) commissioned a project to refurbish eight teaching hospitals which was later upgraded to 14.[3-5] The objective of this paper is to assess the functional status of 10 frequently used equipment in anesthesia and intensive care units among the beneficiaries.
MATERIAL AND METHODS
A structured questionnaire was sent to heads of anesthesia departments in the 14 beneficiary hospitals of the FGN intervention. The questionnaire had a section on basic information about the hospital; number of beds in the wards, number of ICU beds, and number of operating rooms. Another section on the installation of the equipment including end user training. The last section was on scheduled preventive maintenance and repair. They reported on the status of 10 equipment commonly used by anesthetists in the operating rooms and intensive care units. The selected equipment were anesthetic machines, ICU ventilators, defibrillators, patient monitors, central patient monitors, infusion pumps, syringe pumps, arterial blood gas analyzers, and blood/infusion warmers. Key informant interview was also carried out on phone for clarification. Results are presented in frequency tables and graphs.
RESULTS
Questionnaires were sent to a total of 14 teaching hospitals that benefited from the procurement of hospital equipment by VAMED Engineering Company, but responses were returned from 12 (85.7%) out of the 14 beneficiary hospitals. The numbers of 10 most frequently used anesthetic and intensive care unit equipment procured (i.e., anesthetic machine, ICU ventilator, defibrillator, patient monitor [theater], central patient monitor [ICU], patient monitor [ICU], infusion pump, syringe pump, arterial blood gas analyzer, and blood infusion warmer) in each of the 12 teaching hospitals are shown in Figures 1 and 2. The 12 teaching hospitals were coded as facilities A to L for the purpose of anonymity. The average number of beds was 652 (400–800). Operating suites were 11 (8–14) and ICU beds 6.5 (4–9). All equipment were installed between 6 and 17 years (mean 9.75) before the evaluation. The engineering company had camps in each of the hospitals with the following teams; installation team, training team, and maintenance team. There was also a 5-year maintenance agreement for each hospital.
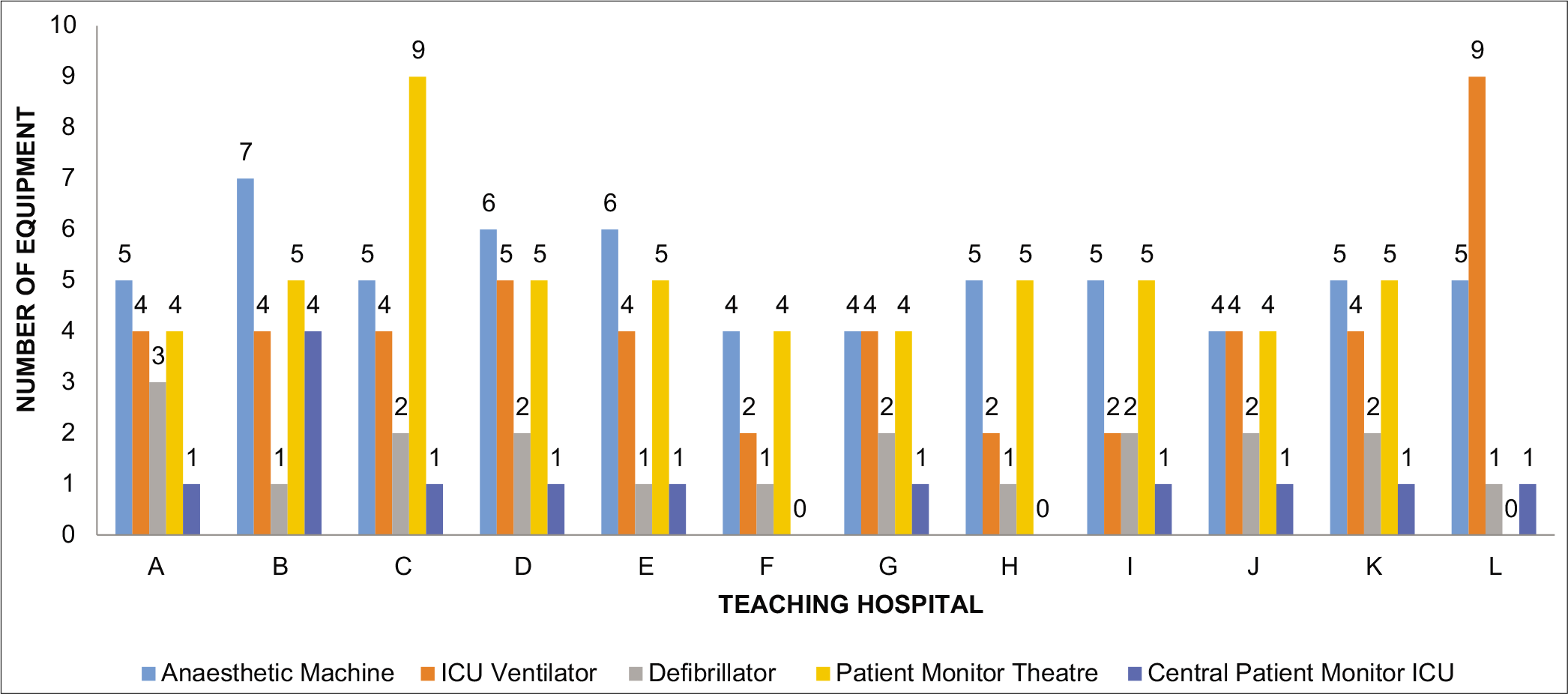
- A multiple bar chart showing the numbers of procured anesthetic machines, ICU ventilators, defibrillators, patient monitor (theaters), and central patient monitor (ICU) across 12 VAMED supported teaching hospitals in Nigeria.
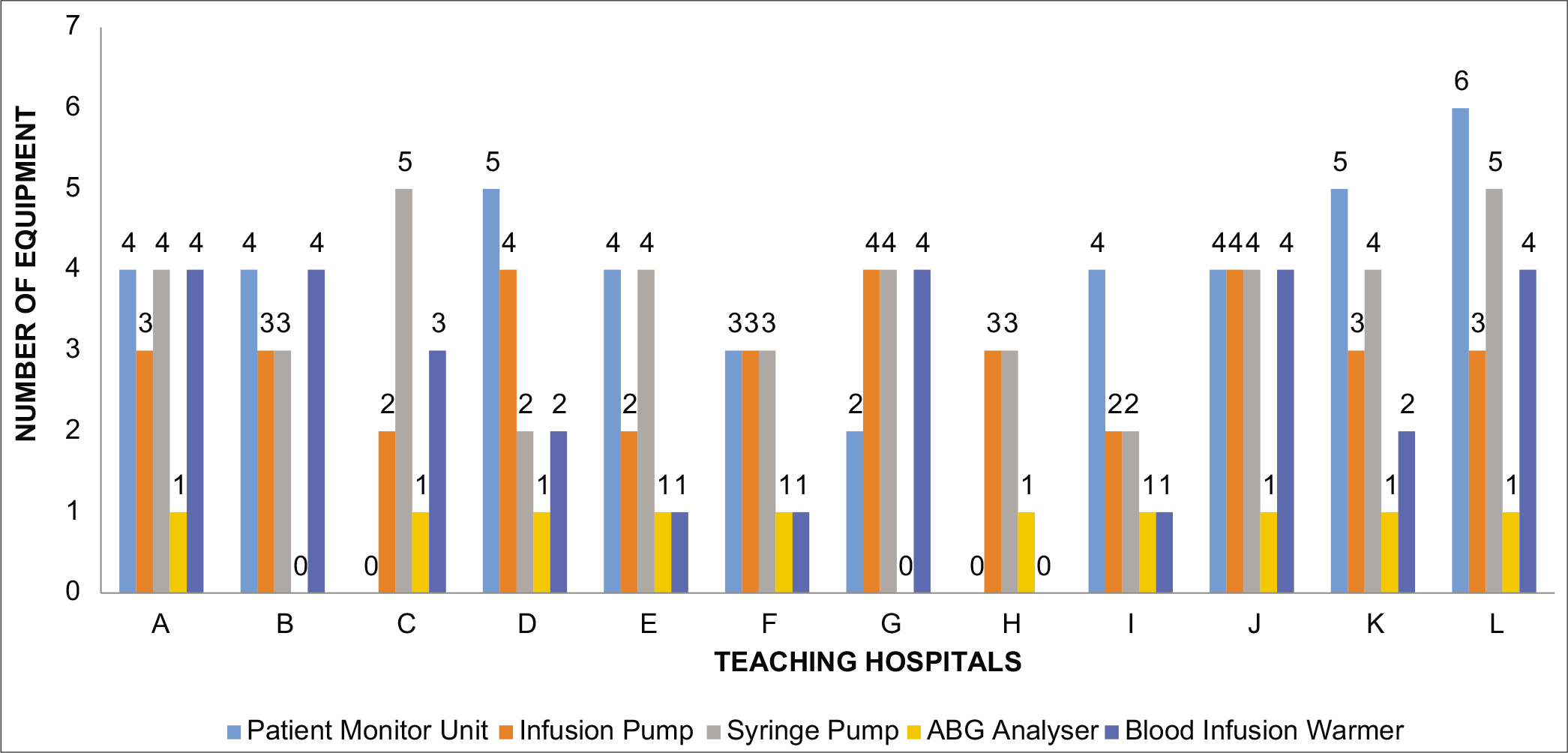
- A multiple bar chart showing the numbers of procured patient monitor (ICU), infusion pump, syringe pump, ABG analyzer, and blood infusion warmer across the 12 VAMED supported teaching hospitals in Nigeria.
The ranges of the number of equipment supplied across each of the 12 VAMED supported teaching hospitals were 4–7 anesthetic machines, 2–9 ICU ventilators, 1–3 defibrillators, 0–9 patient monitors (theater), 0–4 central patient monitors (ICU), 0–6 patient monitors (ICU), 2–4 infusion pumps, 2–5 syringe pumps, 0–1 ABG analyzer, and 0–4 blood infusion warmers.
Functional status of procured equipment in the VAMED supported Teaching Hospitals in Nigeria
The functional status of the equipment procured across the VAMED supported teaching hospitals was audited and graded as fully functional (F), faulty but in use (FU), and spoilt (S). As shown in Figure 3, the responses from each of the supported teaching hospitals showed that overall, the equipment with the relative highest number of fully functional units in all the teaching hospitals is the defibrillator (45.0%), followed by the blood infusion warmer (43.3%), syringe pump (15.9%), infusion pump (13.9%), and patient monitor (theater) (10.9%).
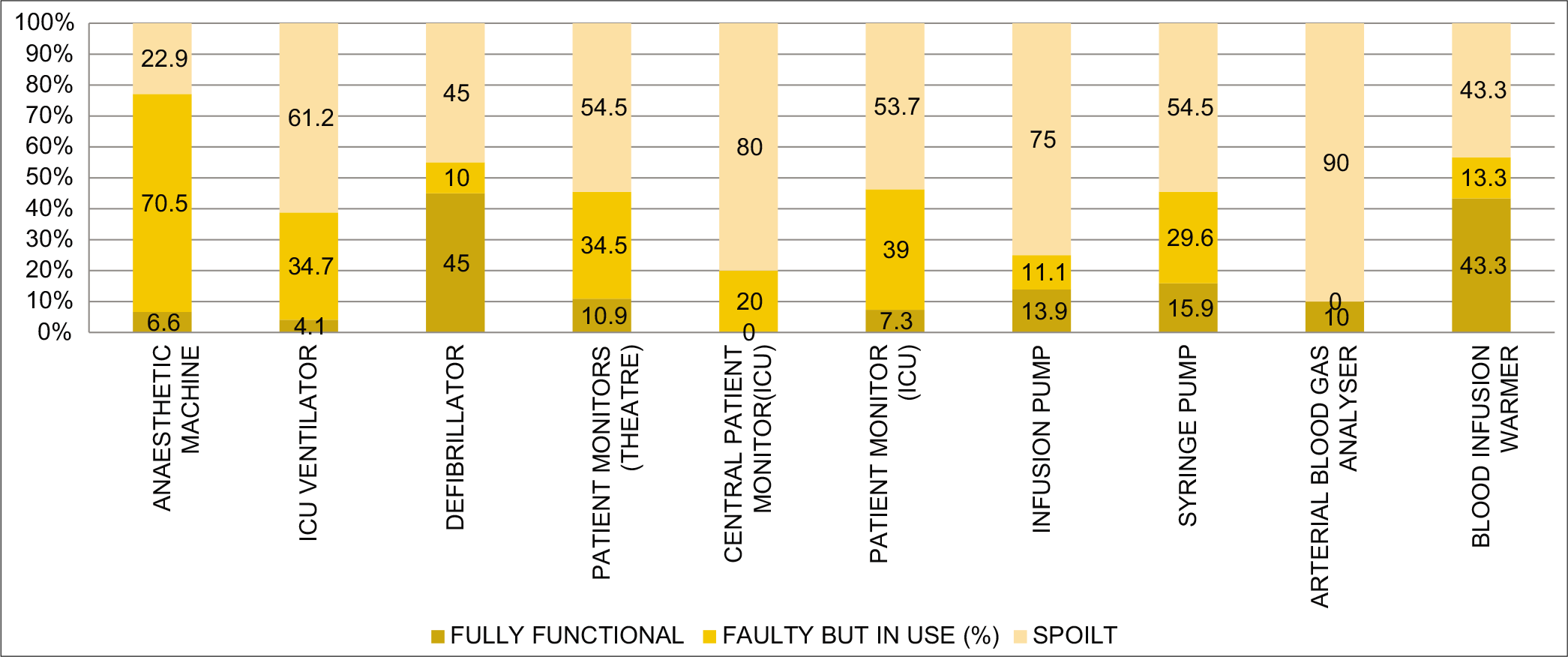
- A composite bar chart showing the relative frequencies of the overall functional status of each type of the 10 frequently used anesthetic and ICU equipment in the 12 VAMED supported teaching hospitals in Nigeria.
The remaining equipment had limited relative numbers of fully functional units left, ranging from 0% (central patient monitor) to 10% (arterial blood gas analyzer). The anesthetic machine had the highest relative number (70.5%) of faulty units that are still in use followed by patient monitor (ICU) (39.0%), ICU ventilator (34.7%), patient monitor (theater) (34.5%), syringe pump (29.6%), central patient monitor (ICU) (20.0%), blood infusion warmer (13.3%), infusion pump (11.1%), and defibrillator (10.0%). The arterial blood gas analyzer had no unit that was faulty but was still in use. Conversely, the equipment with the highest relative numbers of spoilt units in all the teaching hospitals was the arterial blood gas analyzer with 90% of the supplied units already faulty. This was followed by the central patient monitor (80%), infusion pump (70.0%), ICU ventilator (61.2%), patient monitor (theater), and syringe pump (54.5% each), patient monitor ICU (53.7%), defibrillator (45.0%), blood infusion warmer (43.3%), and anesthetic machine (22.9%).
The overall relative frequencies of the functional status of all the supplied equipment were also explored in each of the supported teaching hospitals, as shown in Figure 4. The teaching hospital that had the highest relative number of fully functional units of all the equipment supplied is facility H (70.0%), followed by facility I (28.0%), facility A (27.3%), facility D (15.2%), facility G (13.8%), and facility L (11.4%). The rest of the teaching hospitals had relative numbers of fully functional units of all the supplied equipment <10%; ranging from 0% (facility F) to 6.9% (facility E). However, facility E had the highest relative numbers (82.6%) of faulty equipment that were still in use followed by facility I (56.0%), facility J (53.1%), facility L (42.9%), facility K (37.5%), facility C (34.4%), facility B (29.0%), facility H (25.0%), facility G (13.8%), facility A (12.1%), facility F (9.0%), and facility D (3.0%). Furthermore, the teaching hospital with the highest relative number (90.9%) of spoilt equipment was facility F, followed by facility D (81.8%), facility G (72.4%), facility B (67.8%), facility C (65.6%), facility A (60.6%), facility K (56.2%), facility L (45.7%), facility J (40.6%), facility I (16.0%), facility E (10.3%), and facility H (5.0%).
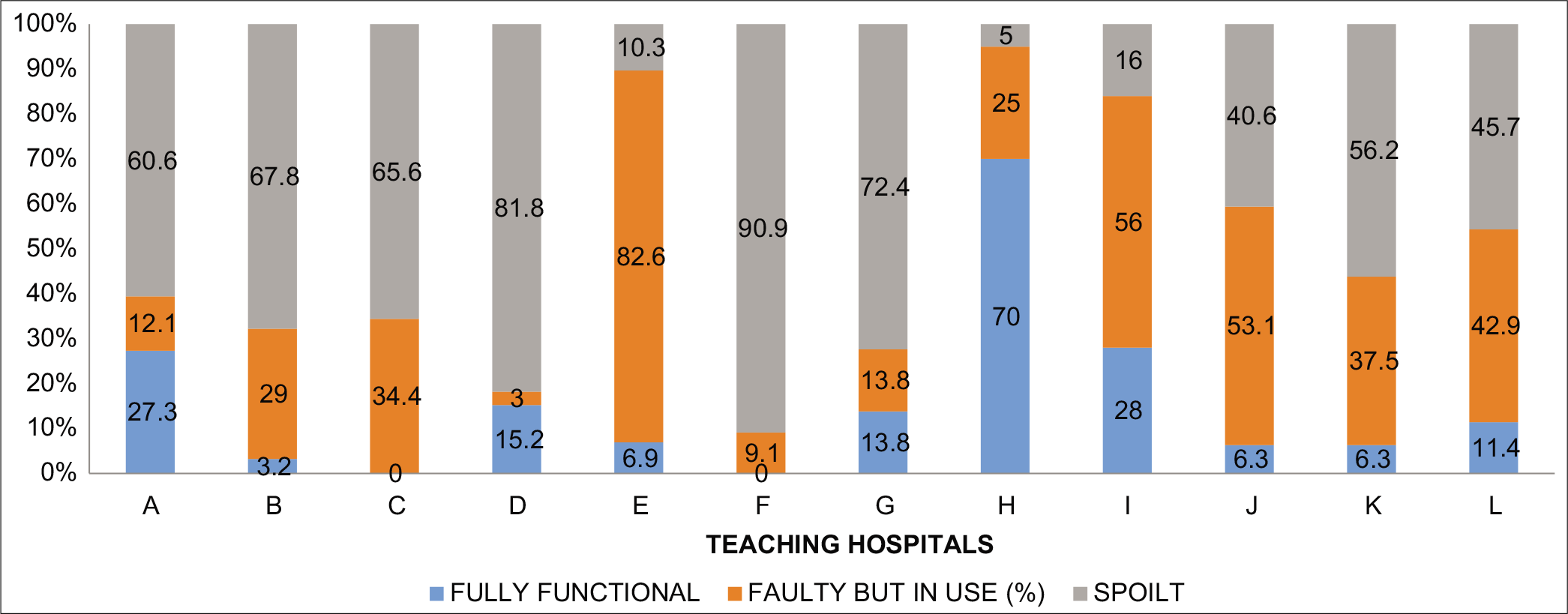
- A composite bar chart showing the overall relative frequencies of the functional capacities of all the supplied equipment in each of the 12 VAMED supported teaching hospitals in Nigeria.
Maintenance practices across the VAMED supported Teaching Hospitals in Nigeria
Maintenance practices across the 12 VAMED supported teaching hospitals were assessed in terms of the average number of preventive maintenance services carried out per equipment per year of use in comparison with the recommended standard of two preventive maintenance services per equipment per year. An average number of preventive maintenance practice that is <1/equipment/year is considered suboptimal, average number of preventive maintenance practice of 1/equipment/ year is considered as fair, while an average number of preventive maintenance practice of ≥2 is considered optimal. The result as summarized in Table 1 showed that out of the 11 teaching hospitals that responded to questions on the preventive maintenance practices, only 1 (9.1%) teaching hospital (facility F) reported that optimal average number of preventive maintenance practice was carried out on each of the supplied equipment per year of use. The remaining 10 (90.9%) teaching hospitals reported suboptimal average number of preventive maintenance practice per supplied equipment per year use as shown in Figure 5.
| Hospital name | Maintenance practice (no./equipment/year) | Assessment |
|---|---|---|
| A | <1 | Suboptimal |
| B | <1 | Suboptimal |
| C | NA | NA |
| D | 0 | Suboptimal |
| E | 0 | Suboptimal |
| F | ≥2 | Optimal |
| G | <1 | Suboptimal |
| H | 0 | Suboptimal |
| I | <1 | Suboptimal |
| J | <1 | Suboptimal |
| K | <1 | Suboptimal |
| L | 0 | Suboptimal |
NA: Data were not available

- A pie chart showing the proportionate number of the VAMED supported teaching hospitals practicing optimal average number of preventive maintenance per equipment per year.
Reasons for suboptimal functionality of equipment
In total, 14 open-ended remarks were received from all the teaching hospitals about the reasons for suboptimal functional capacity of the supplied equipment over the years. The result as summarized in Table 2 showed that the reasons given for suboptimal functionality of equipment across the 12 VAMED supported teaching hospitals were mostly (42.9%) due to unavailability of equipment parts, followed by non- functional equipment parts (28.6%), obsolete equipment (21.4%), and no reagent (7.1%).
| Reasons for suboptimal functional capacity of supplied equipment | Number of responses | Relative frequency of response (%) |
|---|---|---|
| Non-functional equipment parts | 4 | 28.6 |
| Unavailability of equipment parts | 6 | 42.9 |
| No reagent | 1 | 7.1 |
| Obsolete equipment | 3 | 21.4 |
| Total | 14 | 100.0 |
DISCUSSION
Anesthesia equipment chain of survival in this paper refers to planning, acquisition, maintenance, repair, and disposal. The FGN project was a very laudable one. This is because research has shown that there is a discrepancy between health-care need and the ability to provide safe anesthesia in low/low- middle income countries (LMICs) where poor infrastructure is common.[6] Safe anesthesia depends on effective technology. It enabled many hospitals to render new services and scale up existing ones. Other reasons for acquisition of new equipment include improvement in service efficiency, clinical outcomes, cost benefits, as well as meeting specific standards and reducing risk. Medical equipment life cycle consists of planning, acquisition, delivery and incoming inspection, inventory and documentation, installation and commissioning, user training, monitoring of performance, maintenance, replacement, or disposal.[1] The ability of the respondents to report on the installation and training presupposes that the initial steps in the equipment life cycle were reasonably satisfactory.
It is commendable that respondents reported end user training on the use of these equipment. Operator error is a leading cause of device malfunctioning especially in developing countries.[7] Training should include all of the user staff – clinical and technical staffs. This was done commendably by the engineering company. In-house technical staff ought to become the link between user and supplier and should observe any supplier’s technical staff. This also will provide a learning opportunity for the in-house technical personnel.[1,8,9] Although anesthetic technicians were trained in the various hospitals, it has not translated to good preventive maintenance (PM) or corrective maintenance (CM) of anesthetic equipment. This may be because the training was too short and inadequate or the requirements for the maintenance are not readily available for repairs or replacement of faulty parts. It may be necessary to attach biomedical engineers specifically to each anesthesia department for the sole purpose of maintenance and repair of equipment. This may provide an area of sub-specialization to biomedical engineers in Nigerian tertiary hospitals who mostly operate as pool staff in the works department involved in repairs of any/every hospital equipment. Such sub- specialization will ensure careful attention to the peculiarities of anesthesia equipment. A chain is as strong as its “weakest link” therefore despite the strong clinical capacity offered by the provision of these equipment, technical failure resulting from poor maintenance was its weakness resulting in faulty and non-functional anesthetic equipment. The 5-year maintenance contract soon came to an end and many hospitals clearly could not provide preventive maintenance or repair of the equipment. Conventionally, equipment maintenance is categorized as PM and CM.[10] While PM aims to keep the device as new as possible, CM aims to keep the device as good as before failure as possible. CM is carried out due to a service request. Preventive maintenance requirement, on the other hand, should be written down for each device as a check list and reviewed regularly.[11] Our study reveals that among the 10 commonly used anesthetic equipment across hospitals, only 14% were fully functional, 33.6% were faulty but in use while 54.6% were totally spoilt. This is similar to the previous findings that 40% of medical equipment in LMIC hospitals are out of use compared to <1% in high-income countries.[12] The implication is that many services that were made possible by these equipment are no longer being carried out. In addition, the use of faulty anesthetic equipment exposes patients to risks and less than optimal care. Practitioners and hospitals are also at risk of litigation if errors traceable to faulty equipment occur. Anesthesia is generally said to simulate flying an aeroplane. PM and CM are, therefore, critical steps in the anesthetic equipment chain of survival that must not be ignored. Estimates suggest 30–0thetic equipment chain of survival that must not be ignored. Estimates suggest ocof repair.[13] Studies have also found that 80% of hospitals in the African region struggled to find appropriately experienced engineers.[13,14]
Figure 5: A pie chart showing the proportionate number of the VAMED supported teaching hospitals practicing optimal average number of preventive maintenance per equipment per year.
All medical devices reach the point in their life where the cost-benefit ratio goes to the negative because of decreased reliability, increased downtime, safety issues, compromised care, increased operating costs, changing regulations, or simply obsolescence.[15] Unfortunately, many hospitals in the developing countries have become medical equipment graveyards[16] for donor as well as unserviceable equipment. This should not be the case. Disposal of equipment must follow safety procedures to protect people and the environment. A lot of planning must have gone into the acquisition of these equipment. The manufacturers were all reputable companies such as Draeger, GE, Siemens, BBraun, Bayer, Abbott, Philips, Biegler, NEC. This supports previous studies that most medical equipment used in LMIC are produced in high-income countries.[12,17] There is a need for local manufacturers to rise to the challenge of producing suitable equipment for low-resource settings. If this can be accomplished, spare parts will be readily available, and PM and CM will no longer pose a challenge for such equipment. Development of functional partnerships and guidelines as well as consideration of environmental peculiarities such as electricity voltage and availability are proven interventions for equipment survival.[18-20]
CONCLUSION
The government can routinely undertake completion of the chain of survival by sustaining maintenance, repair, and replacement of obsolete equipment – centrally by engagement of maintenance teams from supplier companies. There should be proper training of local biomedical engineers and anesthetic technicians on the maintenance of procured equipment by the companies as part of the equipment contract. Local manufacturers should rise to the challenge of medical equipment production, supply, and maintenance. Routine scheduled preventive maintenance and the constant availability of trained and skillful biomedical engineers will no doubt increase the lifespan of anesthetic equipment and complete their chain of survival.
Declaration of patient consent
Patient’s consent not required as there are no patients in this study.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- A novel approach for healthcare equipment lifespan assessment. Int J Adv Life Sci. 2016;8:1-15.
- [Google Scholar]
- Part 1: Executive summary: 2015 American heart association guidelines update for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2015;132:S315-67.
- [CrossRef] [PubMed] [Google Scholar]
- Available from: https://www.google.com/guardian.ng/refurbishing-tertiary-hospitals-in-nigeria [Last accessed on 2019 Aug 23]
- Available from: https://www.vanguardngr.com/2011/12/transforming-healthcare-delivery-in-nigeria [Last accessed on 2019 Aug 23]
- Available from: https://www.vamed.com [Last accessed on 2019 Aug 23]
- Anaesthetic equipment in low and low-middle income countries. Anaesth Intensive Care Med. 2019;20:518-21.
- [CrossRef] [Google Scholar]
- The Effective Management of Medical Equipment in Developing Countries. A Series of Five Papers. FAKT Project No. 390, Stuttgart, Germany
- [Google Scholar]
- Maintenance management of medical equipment in hospitals. Ind Eng Lett. 2012;2:5-19.
- [Google Scholar]
- Reliability and Maintenance of Medical Devices [Ph D. Thesis]. Toronto, Canada: University of Toronto; 2011.
- [Google Scholar]
- Two different maintenance strategies in the hospital environment: Preventive maintenance for older technology devices and predictive maintenance for newer high-tech devices. J Healthc Eng. 2016;1:1-16.
- [CrossRef] [PubMed] [Google Scholar]
- A New Approach for Preventive Maintenance Prioritization of Medical Equipment, IFMBE Proceedings; 2014. p :41.
- [CrossRef] [Google Scholar]
- Global surgery 2030: Evidence and solutions for achieving health, welfare, and economic development. Lancet. 2015;386:569-624.
- [CrossRef] [Google Scholar]
- International survey on the practice of clinical engineering: Mission, structure, personnel, and resources. J Clin Eng. 2000;25:269-76.
- [CrossRef] [Google Scholar]
- Technology management: A perspective on system support, procurement and replacement planning. J Clin Eng. 1992;17:129-36.
- [CrossRef] [PubMed] [Google Scholar]
- Medical equipment donation in low-resource settings: A review of the literature and guidelines for surgery and anaesthesia in low-income and middle-income countries. BMJ Glob Health. 2019;4:e001785.
- [CrossRef] [PubMed] [Google Scholar]
- Managing equipment for emergency obstetric care in rural hospitals. Int J Gynaecol Obstet. 2004;87:88-97.
- [CrossRef] [PubMed] [Google Scholar]
- How the THET Partnership Model is Different; Looking Back at Two Years of Medical Equipment Partnerships in African Countries. 2019. London: THET; Available from: https://www.thet.org/resources/1690 [Last accessed on 2019 Aug 23]
- [Google Scholar]
- Guidelines for Medical Equipment, Spare Parts, and Maintenance Services Donation, Palestinian National Authority Ministry of Health. 2014. Available from: http://www.lacs.ps/documentsshow.aspx?att_id=15567 [Last accessed on 2019 Aug 23]
- [Google Scholar]
- Failure mode and effects analysis applied to the maintenance and repair of anesthetic equipment in an austere medical environment. Int J Qual Health Care. 2014;26:404-10.
- [CrossRef] [PubMed] [Google Scholar]




