
Translate this page into:
Utilization of obstetric ultrasonography and findings in a cottage hospital in Nigeria

*Corresponding author: Grace Ben Inah, Department of Radiology, University of Calabar, Calabar, Cross River, Nigeria. graceinah2015@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Inah GB, Ngaji AI, Erim AE, Ukweh ON, Fajola AO, Gagar J. Utilization of obstetric ultrasonography and findings in a cottage hospital in Nigeria. Calabar J Health Sci 2021;5:61-5.
Abstract
Objectives:
The integration of ultrasound into routine obstetric workup has transformed antenatal care in resource-poor and remote communities in Africa. The present study aims to investigate the utilization of obstetric ultrasound at a cottage hospital in suburban Nigeria.
Material and Methods:
This retrospective study was conducted at Obio Cottage Hospital, Port Harcourt, Rivers State, South-South Nigeria. Ethical approval was obtained before commencement of the study from the Health Research Ethics Committee of University of Calabar Teaching Hospital with reference number UCTH/HREC/33/533. Reports were retrieved from the records of the radiology unit of the study facility, and data including biometric data and radiological diagnosis were transferred to Microsoft Excel spreadsheet for data analysis. Simple proportions and percentages were used to analyze the data. All statistical analyses were conducted using Statistical Package for the Social Science version 21.0, IBM Inc., Chicago, Illinois, USA. Statistical significance was set at P ≤ 0.05.
Results:
The total ANC visits at Obio Cottage Hospital was 28,072, with 27% (7689) utilization of ultrasound scan. The mean age and range of parity of attendees were 32 ± 2.3 and 1–5, respectively. Of the total scans performed, 99.93% was routine, while 0.07% (5) was clinical-based (targeted). Normal findings were 7520 (97.8%) of antenatal scans recorded, while abnormal cases, multiple gestation, and uncertain diagnosis accounted for 121 (1.57%), 44 (0.57%), and 4 (0.06%), respectively.
Conclusion:
The present study has shown a considerable volume of obstetric ultrasound scan in this cottage hospital, albeit, with low utilization compared to the number of antenatal registration. Findings were mainly normal with minimal need for referral for advance care.
Keywords
Antenatal screening
Ultrasound
Cottage hospital
Pregnancy
Suburban

INTRODUCTION
Maternal mortality remains high in sub-Saharan Africa, and women in remote communities bear the greater brunt of the common pregnancy-associated complications and related deaths.[1-3] Efforts toward containing and mitigating pregnancy-related risks, maternal and child mortality rates are undermined by limited health-care resources and skilled personnel.[4] In recent times, there have been reports on improved pregnancy outcome and reduced maternal and child mortality rates in rural settlements where ultrasound investigation forms part of routine antenatal checks.[2] Ultrasound has gained wide acceptance in medical practice due to its diagnostic efficacy resulting to improved care in many clinical conditions.[5] It is a highly sensitive and affordable imaging device, and many physicians rely on it as first line for most clinical conditions.[6]
With the introduction of ultrasound in obstetrics, surgical interventions have significantly diminished as anatomical structures are visualized in vivo with good definition.[5] Many obstetricians now consider it a part of routine antenatal care,[7] which is useful in assessing fetal well-being and number, gestational age, placental location, pregnancy risk markers, and fetal anomalies.[2,8] A significant majority of women who attend antenatal ultrasound clinic find it interesting and reassuring, especially as it offers improved mother-to-child bonding.[4,9]
The World Health Organization (WHO) has recommended that routine obstetric ultrasound investigation be performed for proper pregnancy dating and identification of high-risk pregnancies[4] and this has since triggered a rise in routine antenatal ultrasound screening in sub-Saharan Africa.[10,11] The alarming rates of pregnancy-related complications including child and maternal mortality in resource-poor and remote communities in Africa[12] emphasize the need to ensure optimal utilization of ultrasound in routine obstetric workups to improve positive perinatal outcome and reduce complications in these regions. The present study aims to investigate the utilization of obstetric ultrasound at a cottage hospital in suburban Nigeria.
MATERIAL AND METHODS
This retrospective study was conducted at Obio Cottage Hospital, Port Harcourt, Rivers State, South-South Nigeria. Obio Cottage Hospital is a 56-bed facility with staff strength of about 160 including 13 doctors and 58 nurses. The facility has an average monthly antenatal visit of 2500 and a delivery rate of about 300 per month. It is one of the health facilities supported by the Shell Petroleum Development Company of Nigeria Limited and its joint venture partners (SPDC JV), through its Regional Community Health Unit and runs a successful Community Health Insurance Scheme that is in partnership with the four industrial communities and the Rivers State government. The scheme has led to an increased utilization of services at the facility due to its affordable, accessible, and quality health services. Some of its obstetric and pediatric services are rendered by medical officers under the supervision of a consultant obstetrician and a pediatrician on sabbatical with SPDC JV who are seconded to the community health facility. The health-care center is equipped with facilities to handle obstetric and gynecological cases. One of such installations is a portable Mindray ultrasound device fitted with a 3.0M Hz curvilinear probe. Ethical approval was obtained before commencement of the study from the Health Research Ethics Committee of University of Calabar Teaching Hospital with reference number UCTH/HREC/33/533.
Reports were retrieved from the records of the radiology unit of the study facility. Data extracted included all obstetric ultrasound scan reports between January and December, 2019. Data were transferred onto a Microsoft Excel spreadsheet for data analysis. Mean age and parity range of antenatal ultrasound attendees were estimated for the study. Pie charts were used to present the frequency of utilization of antenatal ultrasound out of the total antenatal registrants, and the proportion of ultrasound utilization based on routine and clinical needs. Number of antenatal ultrasound findings was presented using a bar chart, while abnormal findings were presented in simple table. Data were further stratified into three groups (15-24; 25-34; and ≥ 35 years) according to maternal age and pregnancy trimester to determine frequency of utilization per group. Simple proportions and percentages were used to analyze the data. All statistical analyses were conducted using Statistical Package for the Social Sciences version 21.0, IBM Inc., Chicago, Illinois, USA. Statistical significance was set at P ≤ 0.05.
RESULTS
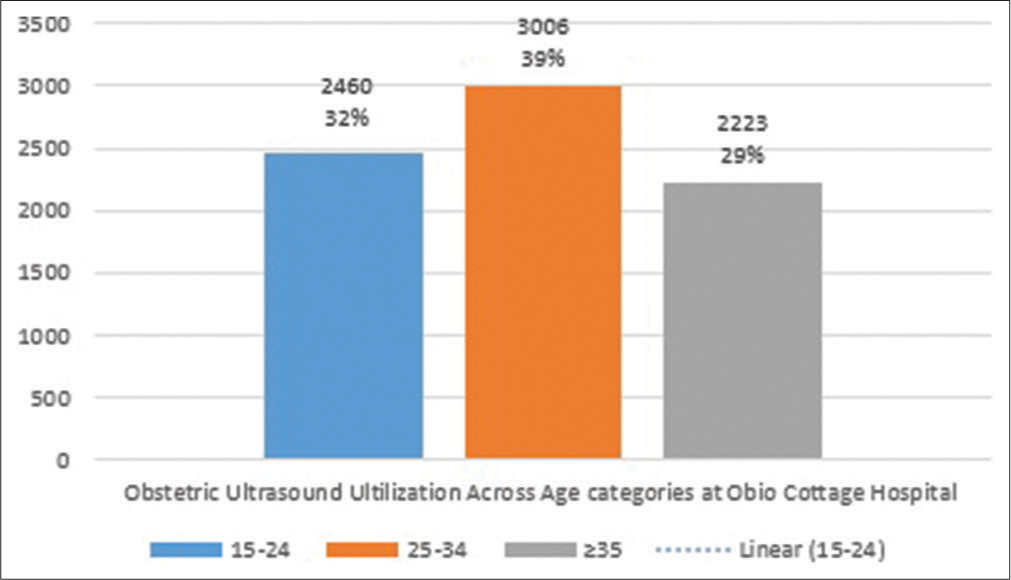
The total ANC visit at Obio Cottage Hospital was 28,072, with 27% (7689) utilization of ultrasound scan [Figure 1]. The mean age and range of parity of antenatal ultrasound attendees were 32 ± 2.3 and 1–5, respectively. Of the total number of scans, 99.93% (7684) was routine, with 0.07% (5) scans as clinical based (targeted) [Figure 2]. Normal findings were 7520 (97.8%) of antenatal scans recorded, while abnormal cases, multiple gestation, and uncertain diagnosis accounted for 121 (1.57%), 44 (0.57%), and 4 (0.06%), respectively [Figure 3]. Out of the total scans performed, women in 25–34 age category accounted for 3006 scans, which ranked the highest (P < 0.05), followed by expectant mothers in the age group of 15–24 (2460). Attendees ≥35 accounted for 2223 of the total scans performed [Figure 4]. Gestational ages recorded were between 6 weeks and 39 weeks, with scans in the first, second, and third trimesters totaling 1161, 3345, and 3183, respectively [Table 1]. Breech presentation 59 (44.1%) and transverse lie 48 were the most common abnormal findings (43.2%) [Table 2].

- Utilization of obstetric ultrasound scan in Obio Cottage Hospital.
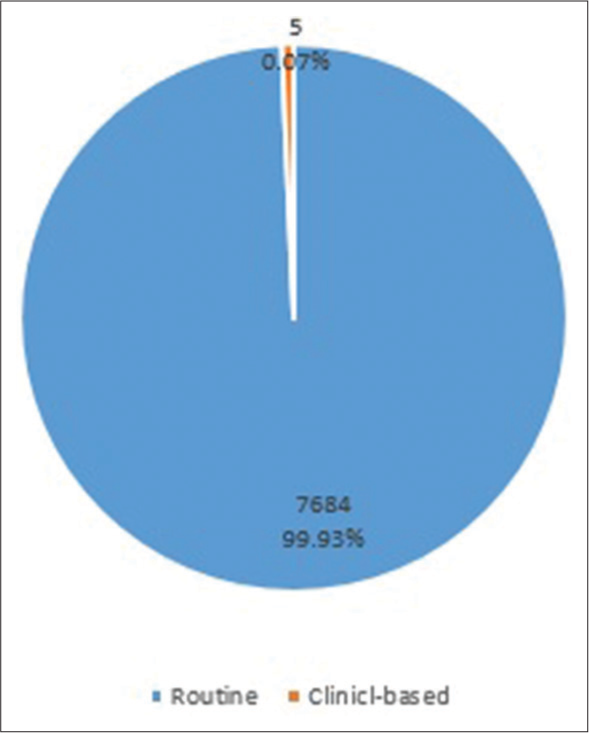
- Reasons for utilization of ultrasound.

- Frequency of obstetric findings in the study.
- Utilization of obstetric ultrasound scan in Obio Cottage Hospital
| Trimester | Number of antenatal scans | Percentage |
|---|---|---|
| First | 1161 | 15 |
| Second | 3345 | 44 |
| Third | 3183 | 41 |
| Total | 7689 | 100 |
| Frequency | Percentage | |
|---|---|---|
| Breech | 59 | 44.1 |
| Transverse lie | 48 | 43.2 |
| Missed abortion | 9 | 8.1 |
| Anembryonic gestation | 5 | 4.5 |
| Total | 121 | 100.0 |
DISCUSSION
Antenatal ultrasound screening has significantly transformed perinatal outcome in a large number of cases in many developing settings.[4,13] In Obio Cottage Hospital, there is a scheme, which provides opportunities for expectant mothers to uptake antenatal ultrasound screening three times during pregnancy: first at booking, then at the second and third trimesters in line with international recommendations. While aiming at improving uptake of antenatal ultrasound screening, operator’s competence and meaningful outcomes are critical points to consider.[14] Our study revealed a low uptake of antenatal ultrasound screening with just 27% out of 28,072 registrants at the facility. Factors such as finance and proximity to facility on the part of the expectant mothers, delayed medical consultations, increased waiting time, and staff attitude could have been the reasons for the low utilization of ultrasound in antenatal visits.[15,16] The impact of this low ultrasound utilization in pregnancy can be linked to a high incidence of negative perinatal outcomes from poor monitoring as suggested by respondents in a survey by Ekott et al.[15] Routine antenatal ultrasound scan accounted for 97% of scan performed in this facility. This means that utilization of ultrasound in this study was largely routine based, with clinically relevant (risk based) scan accounting for only five out of a total of 7689. Sotiloye[17] and Partridge and Holman[18] had argued that perinatal outcomes do not change with number of antenatal visits. In their opinion, obstetric ultrasound scan should be risk based rather than a routine. However, a recent WHO publication has emphasized the need for women to uptake antenatal ultrasound routinely,[4] suggesting that routine ultrasound screening has potentials to detect risk early and women can benefit from intervention and advanced care for a positive perinatal outcome. Up to 97% of scans in the present study were normal, with minimal cases of abnormal findings and uncertain diagnosis (0.06%) which needed referral for specialized care. The observed low rate of referrals may probably be due to the low uptake of antenatal ultrasound screening noted in our study.
While most of the scans were done in mothers aged 25– 34 years (39%), mothers ≥35 years had the least number of ultrasound scan (29%). Meh et al.[2] reported that maternal age was one of the major factors affecting maternal mortality rate and teenage mothers expressed greater odds of maternal mortality compared to older mothers. The reasons for such higher odds have been linked to poor health-seeking attitude in this group and the stigma of unwanted pregnancies,[2] which may have accounted for the lower number of attendances noted by the index study, in this group. Our observation in this regard is similar to that of Meh et al.[2] as lowest utilization was in ≥35 years. Utilization of ultrasound according to trimester showed a preponderance of uptake of scans in second trimester, (43.5%), while the first and third trimesters accounted for 15.1% and 41.4% of the scans performed. The observed low uptake of the first trimester scan in the study suggests that expectant mothers may not have seen early antenatal ultrasound check as very useful, and some in a previous study by Ekott et al.[15] and Umeora et al.[19] regarded frequent scan as being unnecessary, especially in early-stage pregnancy. Expectant mothers rather visit antenatal clinic at the late stage of pregnancy, as most of them are unaware of the purpose and the right time to attend antenatal clinic. In addition, financial constraint was underpinned in their study as a factor bringing about late registration.[20] In a study conducted by Ekott et al.[15] in Obio Cottage Hospital on the need for reduced or focused antenatal visits based on survey, it was observed that reduced visits were acceptable in about 75% of the women. The importance of the first trimester scan cannot be overstated as it allows for early identification of ectopic pregnancies and possible markers for high-risk pregnancies.[15,21] To improve the uptake of early antenatal ultrasound screening, there is a need to educate women in this region on the enormous benefit of early antenatal ultrasound examination. Kim et al.[13] noted that an accurate gestational age estimation is determined by an early ultrasound examination and common causes of maternal mortality including abortion and gestational trophoblastic disease can be detected in the first trimester ultrasound scan.[22] Breech presentation ranked the highest (44.1%) among abnormal findings followed by transverse lie (43.2%), missed abortion (8.1%), and anembryonic gestation (4.5%). Our findings were in discordance with the results of Stanton and Mwanri[22] who reported the most common pathology in their study to be spontaneous abortion, fetal demise, and low-lying placenta.[22] A study by Joseph et al.[21] showed a higher incidence of breech presentation than the present study. This variation probably reveals differences in practice as some centers report fetal mal-presentation even in the second trimester. The large volume of antenatal registrants at Obio Cottage Hospital may have hindered critical and thorough obstetric sonographic readings. Thus, there is a need to employ more sonographers to reduce the workload. One of the limitations of this study is that extracted data did not include useful information on perinatal outcomes and deliveries. However, further study is recommended to address the lapses and provide more comprehensive data.
CONCLUSION
This study shows a high volume of obstetric ultrasound scan in this cottage hospital, however, low utilization compared to the number of antenatal registrations. Findings were mainly normal with minimal need for referral for advanced care.
Acknowledgments
The authors wish to extend their gratitude to Professor Emmanuel E. Ekanem of the Department of Paediatrics, University of Calabar Teaching Hospital for his unrelenting support and encouragement during the course of this work.
Declaration of patient consent
Patient’s consent not required as patients identity is not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Factors promoting or inhibiting normal birth. BMC Pregnancy Childbirth. 2018;18:241.
- [CrossRef] [PubMed] [Google Scholar]
- Levels and determinants of maternal mortality in northern and southern Nigeria. BMC Pregnancy Childbirth. 2019;19:417.
- [CrossRef] [PubMed] [Google Scholar]
- Routine ultrasound in late pregnancy (after 24 weeks' gestation) Cochrane Database Syst Rev. 2015;15:CD001451.
- [CrossRef] [PubMed] [Google Scholar]
- Recommendations on Antenatal Care for a Positive Pregnancy Experience. 2017. Geneva: World Health Organization; Available from: http://www.who.int/reproductivehealth/publications/maternal_perinatal_health/ancpositive-pregnancy-experience/en [Last accessed on 2017 Sep 21]
- [Google Scholar]
- Utilization of antenatal ultrasound scan and implications for caesarean section: A cross-sectional study in rural Eastern China. BMC Health Serv Res. 2012;12:93.
- [CrossRef] [PubMed] [Google Scholar]
- Who should perform the ultrasound examination in gynaecology? Obstet Gynecol. 2012;14:237-42.
- [CrossRef] [Google Scholar]
- Maternal perspectives of prenatal sonogram in a north-eastern population in Nigeria. Libyan J Med. 2009;4:140-2.
- [CrossRef] [PubMed] [Google Scholar]
- Factors influencing referrals for ultrasound-diagnosed complications during prenatal care in five low and middle income countries. Reprod Health. 2018;15:204.
- [CrossRef] [PubMed] [Google Scholar]
- Fetal imaging and diagnosis services in developing countries-a call to action. Trop J Obstet Gynaecol. 2019;36:1-7.
- [CrossRef] [Google Scholar]
- Women's views on routine antenatal ultrasound scan in a low resource Nigerian setting. J Clin Diagn Res. 2018;12:21-5.
- [CrossRef] [Google Scholar]
- Health pregnancy, healthy baby: Testing the added benefits of pregnancy ultrasound scan for child development in a randomised control trial. Trials. 2020;21:25.
- [CrossRef] [PubMed] [Google Scholar]
- Reducing maternal mortality in Nigeria: Addressing maternal health services' perception and experience. J Glob Health Rep. 2020;4:e2020028.
- [CrossRef] [Google Scholar]
- Obstetric ultrasound use in low and middle income countries: A narrative review. Reprod Health. 2018;15:129.
- [CrossRef] [PubMed] [Google Scholar]
- Ultrasound physics and knobology In: Simon BC, Snoey ER, eds. Ultrasound in Emergency and Ambulatory Medicine. St. Louis: Mosby; 2004. p. :10-38.
- [Google Scholar]
- Acceptability of focused antenatal care by antenatal clinic attendees in Obio Cottage Hospital, Port Harcourt, Nigeria. Res J Womens Health. 2017;4:1.
- [CrossRef] [Google Scholar]
- Factors affecting utilization of obstetric ultrasound: A study of semi-urban pregnant women in a developing nation. Sahel Med J. 2020;23:82-7.
- [CrossRef] [Google Scholar]
- Ultrasonography: Recommendations for its Appropriate use in Routine Antenatal Care in Nigeria; From Research to Practice Postgraduate Course in Reproductive Health, 3 March-11 April 2003; 2003.
- [Google Scholar]
- Effects of a reduced-visit prenatal care clinical practice guideline. J Am Board Fam Pract. 2005;18:555-60.
- [CrossRef] [PubMed] [Google Scholar]
- Implementing the new WHO antenatal care model: Voices from end users in a rural Nigerian community. Niger J Clin Pract. 2008;11:260-4.
- [Google Scholar]
- Reasons given by pregnant women for late initiation of antenatal care in the Niger Delta, Nigeria. Ghana Med J. 2011;45:132.
- [CrossRef] [Google Scholar]
- Pattern of obstetrics sonographic requests and findings in a referral hospital in north eastern Nigeria. Niger J Sci Res. 2017;16:6.
- [Google Scholar]
- Global maternal and child health outcomes: The role of obstetric ultrasound in low resource settings. World J Prev Med. 2013;3:22-9.
- [Google Scholar]




